INTRODUCTION
Trust, defined as the “willingness to be vulnerable under conditions of risk and interdependence (Rousseau et al., 1998),” is an essential component of any relationship between patients and Academic Medical Centers (AMCs) that provide health care and conduct research. Lack of trust may impact a patient’s willingness to seek care, have open and honest conversations with their provider, or adhere to treatment plans leading to a lower overall quality of care (Musa et al., 2009). Trust is also critical to achieving equitable health care for marginalized communities. Yet, mistreatment and inferior health care in marginalized communities have been well documented across research and health care systems, both historically and presently (Griffith et al., 2021). Given these circumstances, a natural skepticism and lack of trust in AMCs by marginalized populations is common and expected.
One example is the relationship between Duke University/Duke Health and the majority minority community of Durham, North Carolina. The relationship between Duke and the community of Durham has long been marked by a complex history of collaboration and mistrust, shaped by racial, economic, and institutional dynamics. While Duke has contributed significantly to the region’s development, its historical and contemporary practices have also fostered skepticism among many Durham residents, particularly within Black communities.
The roots of this mistrust date back to the early 20th century, when Duke’s expansion displaced Black residents through land acquisitions and urban planning that prioritized institutional growth over community stability (Swan et al., 1927). Redlining practices further entrenched racial segregation. Historically Black neighborhoods like Hayti were designated as “hazardous” while white neighborhoods near Duke were deemed “desirable” (Spivey, 2024). A recent study by Mohottige et al. (2023) found that Durham neighborhoods burdened by structural racism—characterized by low income, high eviction rates, and limited access to health care had significantly higher rates of chronic diseases such as diabetes and kidney disease. These findings underscore the long-term health consequences of systemic inequality, much of which is rooted in historical policies that Duke either benefited from or failed to challenge. Understanding this history is essential for fostering genuine reconciliation, trust, and equitable collaboration moving forward.
Project ENTRUST, a collaborative initiative between Duke Health and community partners in Durham and the surrounding areas, was created to assess and build the community’s trust in Duke Health. Authentic collaboration with the community as research partner was integral to ENTRUST from the beginning of the project through interpretation and dissemination of study results. The origins of Project ENTRUST can be traced back to the actions of a group of concerned community leaders who had longstanding relationships with both community members and Duke Health partners. These community leaders, aware of the community’s lack of trust in Duke’s health care and research, met with Duke Health partners to seek a solution. With the understanding that trustworthiness must be earned (Anderson & Griffith, 2022; Armstrong et al., 2006), and participatory dissemination and authentic engagement are critical to address trust and trustworthiness (Aguilar-Gaxiola et al., 2022; Wilkins, 2018), Project ENTRUST was launched in 2021 to change institutional practice and policy at Duke Health toward a more trustworthy research and health care system.
A well-documented challenge in this type of translational research is the prolonged lag between the generation of scientific evidence and its integration into practice and policy. Estimates of this delay vary, with some scholars suggesting a timeline of 15–17 years (Balas & Boren, 2000; Hanney et al., 2015; Khan et al., 2021), while others report lags exceeding 50 years depending on the topic and outcomes of interest (Morris et al., 2011). Community-based participatory research (CBPR) and other community-engaged approaches aim to reduce this gap by involving those most affected by a health issue alongside other key invested groups from the outset. These methods emphasize co-creation of knowledge and intentional planning for action and impact (Wallerstein et al., 2018; Wallerstein & Duran, 2010).
According to Israel et al. (2012), several key dissemination strategies are effective for CBPR:
-
Hosting community gatherings to share findings, gather feedback, and foster dialogue with community members and invested groups.
-
Creating culturally relevant dissemination materials (e.g., flyers, brochures, videos) tailored to the community’s context and literacy levels to ensure accessibility and relevance.
-
Collaborating with trusted community-based organizations (CBOs) and leaders to facilitate dissemination and ensure messages reach the intended audiences.
-
Empowering community residents with training and resources to serve as ambassadors or peer educators (e.g., town hall meeting facilitators).
-
Organizing events that incorporate presentations, discussions, and interactive activities to disseminate findings and foster community engagement (e.g., town hall meetings).
These community-collaborative strategies challenge traditional top-down dissemination models, promoting transparency, mutual learning, and empowering communities as agents of change in advancing health equity and research impact (Israel et al., 2012).
The designing for dissemination approach emphasizes the importance of planning for dissemination early in the research process, engaging community partners and stakeholders to identify appropriate formats and timelines for sharing findings and cultivating strong relationships with research end-users throughout the study. These strategies are considered essential for addressing the persistently low rates of dissemination and impact in public health research (Gollust et al., 2025). Grounded in CBPR principles (Wallerstein et al., 2018) and the Truth, Racial Healing, & Transformation (TRHT) framework (W. K. Kellogg Foundation, Revised 2024), Project ENTRUST sought to build trust through dialogue and innovative collaboration with the community from inception through results interpretation and dissemination and integration into institutional practice and policy changes at Duke Health.
The Project ENTRUST Model
There have been few published frameworks or trainings to guide community-engaged research teams in proactively planning impactful dissemination activities (Brownson et al., 2013; Cunningham-Erves et al., 2020, 2021; Kwan et al., 2022). One such framework, the ENTRUST model, was previously described in Barrett et al. (2026) building from Barrett (2021). In brief, the Project ENTRUST Model (see Appendix A) details the 7-phase process of community-engaged participatory research, results interpretation, participatory dissemination, and systems-level change used to build trust in Duke Health.
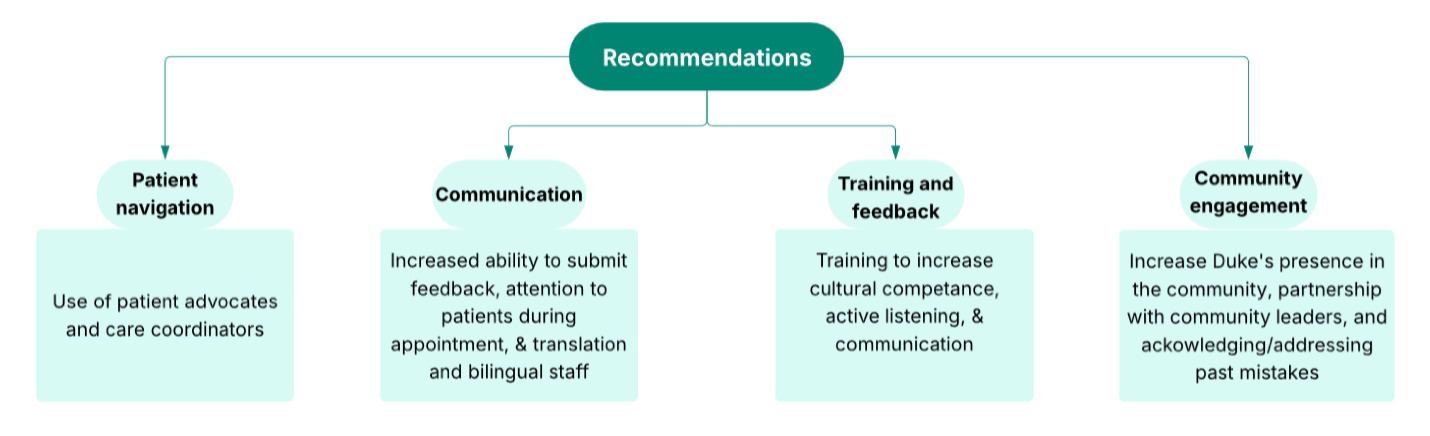
In Phase 1, project leaders engaged with the community to hear concerns and challenges through collaborative community consultation studios (CCSs)(Duke Clinical & Translational Science Institute, 2019, 2026c), meetings to hear directly from community members and listen to their concerns. The ENTRUST team also reached out to institutional leaders to establish buy-in and commitment to change. In Phase 2, project leaders used insights from Phase 1 CCSs to identify domains of community concerns and gather input from scholars across clinical care, health equity, research, and social justice. With the domains of community concern identified, phases 3 and 4 involved further CCSs focused on community members’ lived experiences with Duke Health to create recruitment materials, the ENTRUST Survey (See Appendix B), and survey implementation procedures. Phase 5 included community town hall meetings for collaborative data interpretation and dissemination of the ENTRUST Survey results. Phases 6 and 7 of the ENTRUST Model process involved the creation of a Translation to Action Committee in October 2025. The Translation to Action Committee members include key leadership at Duke Health and community partners. Members meet monthly to create an action plan based on the recommendations that surfaced during the town hall meetings. The action plan will be drafted by the end of summer 2026. Committee members who are Duke Health leaders will take the action plans back to their respective teams for implementation in the fall of 2026.
This manuscript focuses on phase 5 of the ENTRUST Model process, community town hall meetings. Our objectives in this manuscript are to detail partner selection, community town hall meeting design and facilitation, training materials, communication tools, and results.
MATERIALS AND METHODS
The Duke Health Institutional Review Board approved this study (Pro00110562) with a waiver of signed informed consent.
The Project ENTRUST Team – Community Partners and the ENTRUST Core Team
Duke Health is centered in Durham, North Carolina, a majority minority city (40.6% White Non-Hispanic (NH); 31.8 % Black NH; 6.1% Asian NH; 5.3% Mixed Race NH; 15.2% Hispanic any race; 1% Native American, Pacific Islander, or Other Race NH; (U.S. Census Bureau, 2024). Representative participation was sought from community members as partners in Project ENTRUST for both the creation and completion of the ENTRUST Survey and participation in community town hall meetings. These community partners included a racially, ethnically, and linguistically diverse group of current and former Duke Health patients, community members who were not patients, representatives from CBOs and community advisory boards, community and faith-based leaders, as well as Duke Health employees. Importantly, choosing to include current patients, former patients, and community members who had never been patients, allowed Duke Health to learn not only about patients’ experiences but also its reputation among those who never chose or no longer choose to use Duke Health services. This representative sample was achieved through the multi-faceted and inclusive recruitment strategies outlined below. For a complete list of ENTRUST community partner organizations, see the acknowledgments.
Project ENTRUST was led by the ENTRUST Core Team including members of the Duke University Research Equity and Diversity Initiative (READI) (Taylor et al., 2025), a research initiative within Duke Health seeking to promote and improve equity in research practices, and Duke Health faculty and staff chosen for their expertise in evaluation, research methodology, community participatory research, and health disparities. The ENTRUST Core Team designed the methodology and oversaw project administration while including community leaders’ insights to ensure the community had a participatory voice throughout. For example, during this process, the ENTRUST Core Team consulted with the local Public Health department and a Community Advisory Council (Duke Clinical & Translational Science Institute, 2026a) through Duke Clinical and Translational Science Institute’s Community Engagement Research Initiative (CERI) team (Duke Clinical & Translational Science Institute, 2026b). This community input helped shape the domains of community concern, survey design, and details of the town hall methodology. For a complete list of ENTRUST Core Team members, see the acknowledgments.
Town Hall Meeting Development and Design
Following the completion and administration of the ENTRUST Survey, Phase 5 of the ENTRUST model focused on developing and implementing community town hall meetings. To design the town hall meetings, a CCS was convened to inform the town hall presentation strategy. The CCS, run by the CERI team, was a 1.5-hour structured, non-research, listening session between the ENTRUST Core Team and local community members to gather community feedback (see Figure 1).
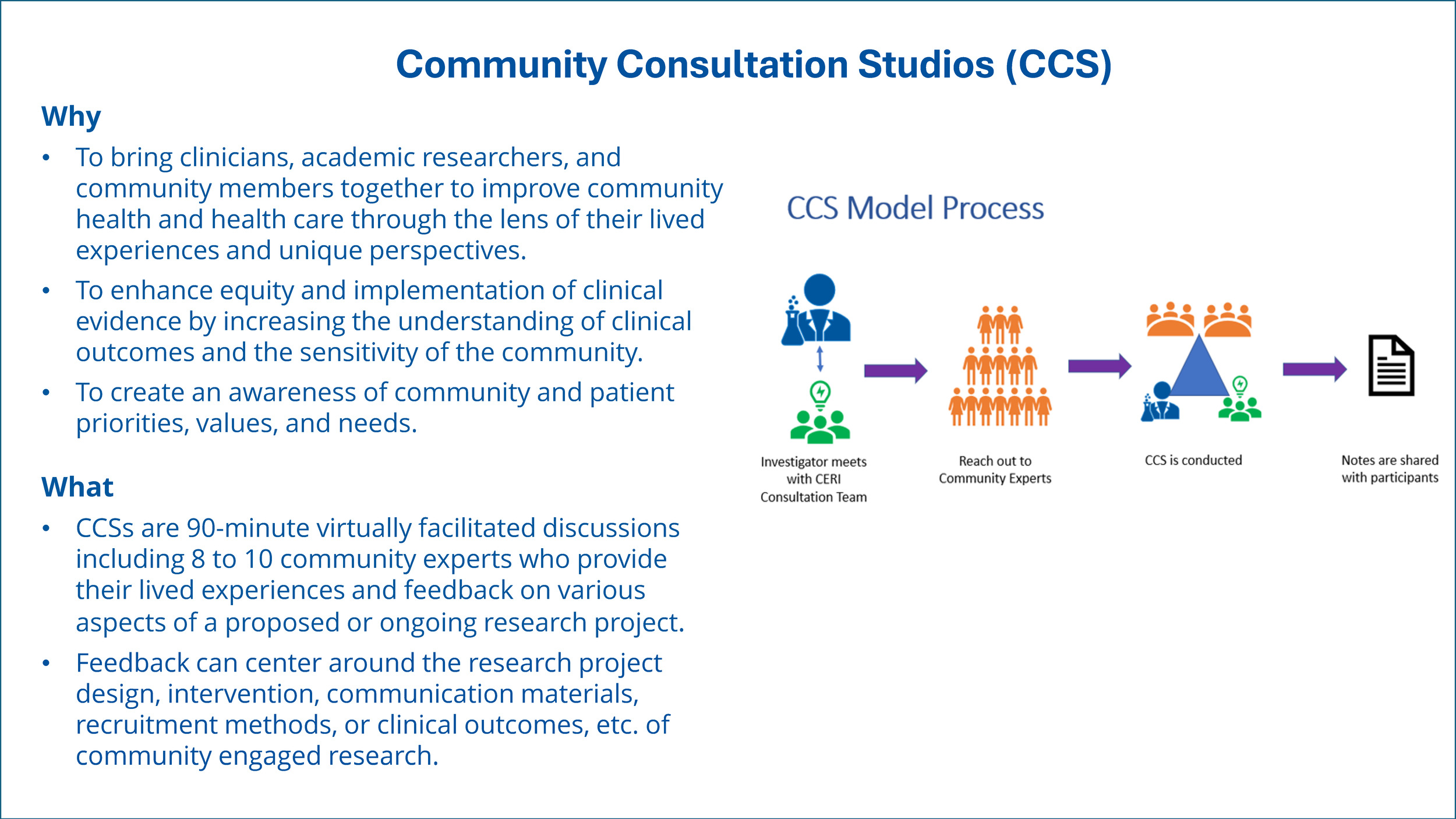
The planning phase for this CCS spanned approximately 4–6 weeks and involved coordination between CERI and 6–10 community members. The ENTRUST Core Team was invited to participate in two preparatory meetings and send two representatives to the CCS, during which they were asked to present a 10–15-minute overview of Project ENTRUST. The ENTRUST presentation included preliminary data visualizations of the ENTRUST Survey findings to solicit feedback and refine the community town hall engagement strategy including slide content and questions to support data interpretation (see Appendix C). The CCS session was attended by nine individuals (three male, six female), ranging in age from their 20s to early 70s. Each participant received a $50 gift card in recognition of their time and contributions. The CCS was guided by a neutral facilitator and supported by 2 impartial staff members from the CERI team who served as note takers. Notes from the session were compiled and returned to both parties (the ENTRUST Core Team and CCS participants) within one week, ensuring transparency and continuity in the feedback loop. This model of engagement reflects a commitment to community-informed research design and equitable collaboration.
Feedback from the CCS was incorporated into the presentation strategy, and survey data was further refined to create the final town hall meeting presentation. The ENTRUST Core Team planned 6 community town hall meetings in both English and Spanish to disseminate and interpret survey results. This phase was grounded in the principle that every individual possesses a valuable perspective that warrants recognition and inclusion. The town hall meetings not only served as venues for sharing project findings but also empowered community members to interpret survey data themselves, challenging conventional research paradigms and positioning the community to inform policy and programmatic decisions.
Town hall meetings were conducted with the four primary groups originally engaged in the ENTRUST Survey: patients and community members (3 virtual town hall meetings), employees (2 town hall meetings, 1 in-person and 1 virtual), and community-based organizations (1 virtual town hall meeting). Here we discuss the utility of community town hall meetings as participatory mechanisms for fostering trust and addressing mistrust among these key constituencies.
The town hall meetings were structured around two central objectives:
-
Critical engagement with survey findings: Participants were invited to examine the ENTRUST Survey data, particularly as it pertained to community trust and perceptions of Duke Health’s trustworthiness in health care and research. Discussions focused on experiences of discrimination and a spectrum of attitudes and beliefs regarding health care delivery and medical research.
-
Community perspectives and strategic recommendations: Participants shared their reactions to the findings and proposed actionable strategies to enhance trust and institutional trustworthiness within Duke Health and its research initiatives.
Recruitment Strategies to Promote Town Hall Participation
To maximize participation, the ENTRUST Team employed a multi-pronged outreach strategy (Appendix D):
-
Institutional dissemination: Information was shared through Duke University and Duke Health system networks, particularly targeting individuals in community-facing leadership roles.
-
Spanish-language accessibility: All materials, including emails and flyers, were translated into Spanish by the Duke Office of Clinical Research.
-
Flyers: Promotional materials emphasized inclusivity with the message: “Survey Results are in! We want to hear your feedback – To hear, to share, and to discuss,” reinforcing the project’s commitment to community voice.
-
Website updates: The Project ENTRUST website was updated with a registration link for the town hall meetings.
-
Event listings: Town hall meetings were posted on Duke’s internal events calendar.
-
Targeted CBO outreach: Invitations were extended to select community-based organizations including the African American COVID Taskforce Plus (AACT +), the Latinx Advocacy Team & Interdisciplinary Network for COVID-19 (LATIN-19), and the Duke Clinical and Translational Science Institute’s CERI team, to support promotional efforts. This CBO sharing method ensured that knowledge of the town hall meeting events would reach populations that might have otherwise been unaware of the opportunity to provide feedback.
-
Social media campaign: Town hall meeting events were promoted via Facebook and Twitter.
The ENTRUST Core Team also collaborated with local media outlets to broaden outreach and encourage participation. Registration links and QR codes were included in all promotional materials and email invitations to facilitate easy access.
Town Hall Meeting Procedures
Registration for town hall meetings was handled through Qualtrics; names and emails were collected to provide potential participants with a link for the virtual meetings or information about attending in-person meetings. Participants were notified during registration and again at the start of the town hall meeting that the session would be recorded, and that by staying in the session, the participant agreed to be recorded. Participation was voluntary, and participants were notified that they may leave the town hall meeting at any time if they did not wish to be recorded.
Town hall meetings were conducted either virtually (using Zoom) or in person, and each session lasted 90 minutes. Participants in the virtual town hall meetings used their own electronic devices to participate and could choose to participate from a location of their choice. Town hall meetings were conducted in both English and Spanish to increase community participation. Unlike typical presentations that are often advertised as presentations in Spanish but are conducted primarily in English with a Spanish translation, the Spanish ENTRUST town hall meeting was conducted primarily in Spanish with dissemination materials also presented in Spanish.
Participants attending virtual town hall meetings were compensated with a $25 gift card. For the Duke employee town hall meetings, participants could opt to enter a raffle for one of 5 $50 gift cards for each employee town hall meeting. Lunch was also provided for each participant at the in-person employee town hall meetings.
A key component of these town hall meetings was training community leaders and members to serve as co-facilitators through a community-researcher dyad program. Potential town hall participants could indicate interest in serving as a facilitator during the registration process; 30 community facilitators were recruited from this method. The ENTRUST Core Team provided 2 training sessions for facilitators introducing them to preliminary descriptive, yet uninterpreted, ENTRUST Survey findings, visualizations, and meeting goals. Facilitator guides in both English and Spanish were provided (Appendix E). Training content included background information, the town hall meeting agenda, role assignments, and 4 guided questions with probing questions for breakout sessions.
Each town hall meeting began with an introduction of everyone attending and presentation of the data. After the initial presentation of data, each town hall meeting split up into 6 to 10 breakout groups with 7 to 10 people each for collaborative group discussion. These breakout sessions were co-led by ENTRUST trained dyads of one community leader and one Duke Health academic/research system staff member. Facilitators read discussion questions and encouraged active participation by inviting participants to share their thoughts (through chat, or by unmuting and talking for virtual sessions). Each breakout room included a designated note-taker responsible for organizing responses by theme, reading aloud chat contributions, and assisting participants as needed.
Breakout discussions were structured around 4 guided questions related to the theme of trust and trustworthiness.
-
Based on the results 18% of respondents stated that patients have been deceived or misled by Duke. What are your thoughts and reactions about this?
-
Based on the results 26% of respondents reported having hesitated or avoided getting health care at Duke. What are your thoughts and reactions about this?
-
We saw from the presentation that 34% of participants report experiencing discrimination. What are your thoughts and reactions about this? Was anything surprising or is this what you expected?
-
Based on the data 21% of respondents felt that a health care provider was not listening to what they were saying. What are your thoughts and reactions about this?
Each question was allotted approximately 10 minutes for discussion.
Facilitators used probing questions to deepen the discussion:
-
Did the data resonate with you?
-
Were you surprised by the data?
-
Do you believe the data accurately represents your community?
-
What actions should Duke Health take to build trustworthiness?
-
What have you heard, seen, or experienced about Duke Health?
-
What steps can Duke Health take to effectively address and change this viewpoint?
Participants were asked to share and respond to questions based on their own lived experiences, as lived experience plays a vital role in building trust, reflects firsthand knowledge gained through life events, and is grounded in personal, emotional, and social realities.
Following the breakout sessions, a 15-minute report-back was conducted in the main room. Facilitators summarized key insights and community recommendations for next steps. Participants were also invited to complete an optional 13 question post-town hall evaluation to collect demographic information and assess the utility of the town hall meeting, satisfaction with the meeting, perceived value of the information presented (see Appendix F). Participation in the town hall meeting was not contingent upon completing the post-town hall evaluation.
RESULTS
Over 300 Durham area community members, CBOs, and Duke Health patients and employees participated in 6 town hall meetings (5 in English and 1 in Spanish) to review and interpret the ENTRUST Survey data. Results below represent findings across all 6 town hall meetings.
Participant Challenges with Duke Health
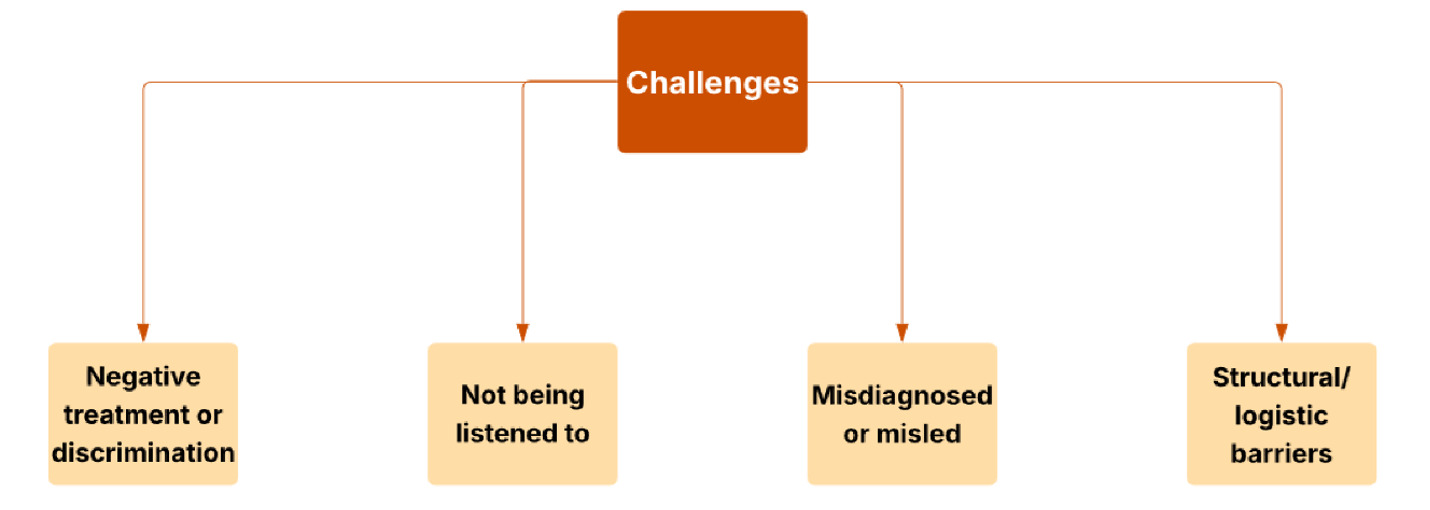
Participants reported varied challenges with the Duke Health system (see Figure 2). Experiences of mistreatment and interpersonal discrimination emerged as recurring challenges that negatively influenced participants’ trust in and engagement with Duke Health. Participants reported this occurring due to race, gender, age, socioeconomic status, sexuality, and health diagnoses. The historical context of racial discrimination in Durham, North Carolina, where Duke University is located, was also mentioned, with several participants noting that past and ongoing racism influences how communities perceive and engage with the health care system. Participants also cited issues of not being listened to or respected; specific examples included providers focused on typing notes over interacting with patients during visits, listening with intent to respond rather than listening to understand the patient’s experience, and drawing conclusions about diagnosis before the patient had finished explaining their symptoms. These concerns were sometimes linked to reported experiences of discrimination occurring among older adults, women, and patients of color. Participants also reported experiences of misdiagnosis, such as receiving major diagnoses without comprehensive testing. Other participants recalled past incidents of research misconduct that damaged community trust and fueled an expectation they would be deceived again. In addition, participants described structural and logistical barriers within the health care system that made care difficult to access or navigate, such as long wait times to get an appointment (especially for new patients and specialized care), feelings of being “practiced on” as Duke Health is a teaching hospital, and the perceived high cost of care.
Participant Recommendations for Duke Health
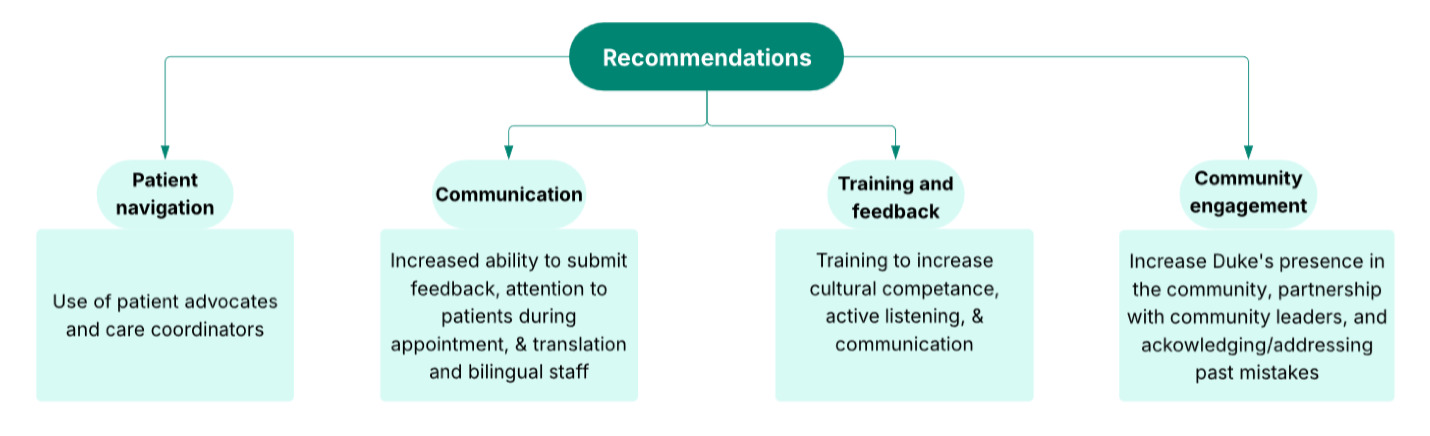
Beyond addressing challenges, participants offered numerous recommendations to improve trust, communication, and care delivery at Duke Health (see Figure 3). Increased attention to and focus on patients during the visit was a key recommendation. Multiple participants suggested the use of patient advocates and care coordinators who could help patients better understand medical information and support their needs, especially for those who may feel overwhelmed, have limited health literacy, or face barriers related to language or power dynamics during appointments. Relatedly, participants encouraged improving communication between patients and providers. During clinical care, participants recommended reducing provider reliance on computers during appointments to improve eye contact and using scribes to facilitate better in-person engagement. Participants supported more visible and accessible channels for feedback, including improved communication channels allowing patients to submit post-appointment feedback or provider-related grievances through patient portals like MyChart. In addition, participants recommended regular and required training programs to improve cultural competence and patient interactions; they reported that these trainings could address how to recognize and reduce discrimination, how to listen actively, and how to communicate clearly and respectfully with patients. Participants also emphasized the need for more diverse staff and providers across all levels, including interpreters and bilingual clinicians, to support improvements in patient interaction. Finally, to build long-term trust, participants strongly emphasized the need for community engagement, including added efforts for Duke Health to be present in the community, partner with community leaders, and address mistrust by acknowledging and addressing past mistakes.
Post-Town Hall Meeting Evaluation
Post-town hall meeting evaluation data (N=121) from all 6 town hall meetings demonstrated consistently positive feedback across multiple domains of participant experience. When asked to rate the overall quality of the event on a scale from 1 (extremely dissatisfied) to 5 (extremely satisfied), 87% of attendees provided favorable ratings (4 or 5), with an average rating of 4.67, suggesting that the format and content were effective in engaging the audience. Participants felt they were able to share their thoughts and concerns during the town hall meeting (average agreement rating of 4.63, with 1 being strongly disagree and 5 being strongly agree). Participants also described the town hall meetings as a meaningful experience (average agreement rating of 4.71), indicating that the meetings provided not only relevant information but also a sense of inclusion and value in the dialogue. Participants felt that the inclusion of the community in interpreting ENTRUST Survey findings was important to build trust in both health care and research (average agreement ratings of 4.85 and 4.77, respectively). Overall, the participants reported that the town hall format was a good forum for improving Duke Health’s trustworthiness (average agreement rating of 4.69).
Qualitative review of the open-ended questions showed that respondents felt it was important to participate in the town hall meetings in order to share their experiences, contribute to improvements in health care, and ensure their voices were included in shaping Duke Health’s future. Many saw the town hall as a platform for transparency, accountability, and community empowerment. When asked how the town hall could be improved, participants suggested improved logistics (e.g. allotted time for breakout discussion, transition to the breakout room), inclusivity, and clearer communication, broader outreach, and more actionable follow-up steps. Participants emphasized accessibility, anonymity, and reaching marginalized voices through creative and community-based methods as important for collaborative community data interpretation. There was a strong desire for Duke Health to demonstrate responsiveness and commitment to change with tangible outcomes and continued dialogue.
DISCUSSION
In 2021, when Project ENTRUST was launched, there was a strong desire from health systems across the nation to address instances of harm involving AMCs. That desire for change, as well as the health consequences of medical and research mistrust, are pressing concerns for health care systems as their primary goal is to heal people. In the ENTRUST town hall meetings, participants emphasized that mistrust is a direct barrier to achieving that goal. Community insights reflect a deep understanding of local needs and offer grounded recommendations for policies and practices that build and repair trust. An important facet of Project ENTRUST was the exploration of innovative approaches to participatory dissemination, emphasizing the active engagement of communities as equal partners in the research process. Guided by CBPR principles, ENTRUST invited the community to review the data and propose their own interpretations of the ENTRUST Survey results, challenging traditional research paradigms by positioning the community as an active partner in the research process.
To ensure broad and inclusive participation in Project ENTRUST’s community town hall meetings, a multi-modal outreach strategy was employed that leveraged digital, print, and community-based channels. Email campaigns and website updates provided direct and accessible registration pathways, while visually engaging flyers translated into Spanish were distributed to reinforce inclusivity and language accessibility. Social media platforms such as Facebook and Instagram amplified visibility and engagement, particularly among younger and digitally connected demographics. Crucially, outreach was strengthened through strategic partnerships with CBOs. Groups like CERI, AACT+, El Futuro, El Centro and LATIN-19 played a vital role in disseminating information and encouraging participation among populations that might otherwise be overlooked.
ENTRUST town hall meetings were structured consistent with best practices around language access, allowing Spanish-speaking individuals to process and share their thoughts in Spanish rather than English. Despite these efforts, only 29 Spanish-speaking individuals (approximately 10% of town hall participants) attended the ENTRUST town hall meeting conducted in Spanish. This experience demonstrates that engaging the Spanish-speaking community in collaborative data interpretation and dissemination requires more individual outreach and a greater partnering with community groups as a bridge to participation—engaging the community in new opportunities requires leaning into these trusted spaces even more.
Qualitative analysis of town hall discussions revealed a complex set of challenges, often seeded in the history of the relationship between the community and Duke Health, affecting the community’s trust in Duke Health. Participants reported both historic and current racial discrimination, a lack of provider attention and respect, and feeling misled or being misdiagnosed leading to erosion of trust. While many of these issues are deeply rooted and difficult to overcome, participants offered clear recommendations for actionable changes Duke Health could make to improve trustworthiness. Many of the proposed recommendations revolved around communication and community engagement, which are core principles of Project ENTRUST.
While the Translation to Action Committee is newly created, community feedback from the town hall meetings has already informed short-term priorities for implementation. Going forward, the Translation to Action Committee has been tasked with realizing the recommendations provided by the community through the town hall meetings. Success for this final step in the ENTRUST process will include increased engagement and partnerships with community leaders. Duke Health will strive to have a more prominent presence in the community, acknowledging and addressing past mistakes while building trustworthy relationships. The Translation to Action Committee will work to establish better, more open communication practices between patients and providers, staff, and the health system including implementing the use of patient advocates and care coordinators. Finally, community informed training efforts in cultural diversity will increase provider and staff cultural competence allowing for more active listening and equitable communication. Implementation efforts will begin in the fall of 2026.
By engaging community members and leaders as collaborative research partners, Project ENTRUST prioritized community voice, thoughts, and lived experience in data interpretation and dissemination. The ENTRUST Survey data was understood through the lens of the community, and disseminated with community, not to the community. Any decisions made by the ENTRUST Core Team without direct involvement of community members, such as the preliminary cleaning and analysis of survey data for presentation at the town hall meetings, were informed by extensive and careful communication with community members and leaders through a CCS or Community Advisory Council. Although we acknowledge that not including community members directly in every part of the project could signal a lack of respect for their knowledge of the community, we also saw a need to carefully balance methodological expertise (e.g., formal analysis training for cleaning data), extra time needed to involve community member in each step, and over burdening community members without providing adequate compensation for their time and efforts.
Our findings suggest that town hall meetings foster inclusive dialogue, enhance transparency, and promote collaborative problem-solving. Evaluation of the town hall meetings showed that this participatory dissemination method is accepted and appreciated by community members. Participants were engaged in the town hall meeting process and reported feeling increased trust in Duke Health after the meeting, highlighting the role of participatory engagement in fostering stronger relationships between communities and health systems. Importantly, many respondents expressed that the town hall meetings contributed to their perceptions of improved care, underscoring the potential of such community-centered forums to positively influence attitudes toward health services. These findings support the utility of town hall-style meetings as a strategy for enhancing communication, building trust, and improving perceptions of care quality within diverse populations.
The core framework of Project ENTRUST as an iterative community collaborative model culminating in participatory interpretation and dissemination of findings to improve a system is broadly translatable to other types of research seeking to improve systems for communities. The key to the Project ENTRUST model is authentic involvement of the community as partner in research through each step of the process. Regardless of context, the first step will always be listening to community concerns. From there, community concerns can inform the development of a research product that will generate information useful to the context. In some cases, a survey may be less appropriate and substitution with a focus group, individual interview, or observation may be a better fit. Whatever research tools are developed through this process, participatory interpretation and dissemination of the findings can lead to actionable, community-informed steps to improve the system.
CONCLUSION
The ENTRUST town hall meeting format demonstrated its value as a meaningful and strategic participatory dissemination tool, designed not only to share findings but to foster dialogue and co-create solutions. Structured around two central objectives—critical engagement with ENTRUST Survey data and the generation of community-informed recommendations—these meetings provided a space for participants to reflect on issues of trust, discrimination, and institutional accountability. The insights shared suggest a deep understanding of local needs and provided grounded strategies to enhance trustworthiness within Duke Health and its research initiatives. Importantly, the feedback gathered during the town hall meetings was instrumental in guiding next steps, including the formation of a Translation to Action Committee and the development of sustainable community-AMC partnerships. As such, the town hall meetings served not only as a platform for dissemination but as a catalyst for institutional change and ongoing collaboration. The participatory dissemination strategies employed by Project ENTRUST provide a model to move not only Duke Health but other AMCs forward toward becoming more responsible and accountable partners in community trust building and health equity efforts.
Corresponding Author
Salimah El-Amin, DrPH, MPH; Duke University; Durham, NC 27701; Phone: (919) 681-5984; Email: salimah.el-amin@duke.edu
Funding
The Project ENTRUST is supported by the Duke Endowment Grant and the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002553. Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number F99AG088695 (PI-Fellow M. D. Green). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests
The authors declare no conflicts of interest.
Ethics approval
The ENTRUST Project was approved by Duke Health’s Institutional Review Board (Pro00110562).
Acknowledgements
We would like to thank those who were central to the work of Project ENTRUST.
Community Partners: Reverend Dr. B. Angeloe Burch, Sr., the African American COVID Taskforce Plus (AACT +), the Latinx Advocacy Team & Interdisciplinary Network for COVID-19 (LATIN-19), El Centro Hispano NC, El Futuro, North Carolina Central University Department of Public Health Education, HealthLit4Wake Health Equity Coalition, Durham Community Health Coalition Inc., Together for Resilient Youth (T.R.Y.) Coalition, AME Zion Health Equity Advocates & Liaisons (AME Zion HEAL), and members of the CTSI Community Engagement Research Initiative (CERI) team – Leatrice Martin, Kenisha Bethea, Daphne Lancaster and Cindy Haynes. We would also like to thank the community members who completed the ENTRUST survey and added valuable insight during the data interpretation town hall forums.
ENTRUST Core team members: Community Engagement Research Initiative (CERI), Center for Equity in Research [EIR], Office of Evaluation and Applied Research Partnership [O-EARP]), Duke Clinical and Translational Science Institute (CTSI), Duke Office of Community Health.
Editorial Support: Terren Green, Medical Editor, Duke Clinical Research Institute, Duke University.