Introduction
Action Research (AR) is a framework for conducting participatory research. Its key elements are that iterative research cycles are conducted in practice, together with relevant stakeholders, while also extending scientific knowledge (Reason & Bradbury, 2007). AR is increasingly used in eHealth studies, which are about the development, implementation, or evaluation of technology in healthcare. This can include a variety of topics, like the prevention of illness through the promotion of healthy lifestyles (e.g., through activity monitoring), self-management of disease (e.g., tracking of symptoms over time), or shifting of care from a clinical setting to the home of the patient (e.g., videoconferencing with healthcare professionals). Additionally, the types of technologies used for eHealth also vary greatly and include things like apps, virtual reality, sensors or robotic devices. Furthermore, what is specific in the context of eHealth is the involvement of various stakeholders with diverse backgrounds. Projects affect and commonly include stakeholder groups like patients, healthcare professionals, or technology developers.
In eHealth research, the cyclical nature of AR and the close connection to daily practice provide many benefits (Hayes, 2014; Oberschmidt et al., 2022). Additionally, AR focuses on actively engaging stakeholders. Studies on “champions,” the drivers of a project who are exceptionally committed to said project, show that such actively participating stakeholders can help the successful implementation of a new service or technology in daily practice (Miech et al., 2018) However, research also points out that AR often requires significant time and resources (Grant et al., 2008). Yet in some cases, through faster-paced studies, it would be possible to quickly and easily determine whether a project has any potential benefit and is worth pursuing further. Additionally, some specific research questions could be (partially) answered in a relatively short period of time to avoid unnecessary delays and disturbances of the work in practice.
Recent studies have suggested so-called flash mob studies as a way of quickly finding answers to questions in daily practice (Moons, 2021). Flash mob studies get their name from the social activities where large groups of people gather in a specific location for a brief period to perform an action together (e.g., dance). In research, this means that data is collected on a large scale (e.g., in multiple locations at the same time, or involving many participants) in a short period of time. Moons (2021) suggests that a core research team sets up the study (e.g., develops material and requests ethical approval) while local partners from daily practice help in recruiting participants and collecting data. Flash mob studies are most suitable for topics and research questions that are “fun, hip, and playful, in order to gain enough interest” (Moons, 2021).
There are only a few examples of flash mob studies in eHealth literature so far, but their results and reflection on the method are promising. Schols and colleagues (2019) found the flash mob study they conducted as part of clinical diagnostic research to be resource - and time-saving compared to more traditional methods. In their analysis of health record data, van Nassau (2021) and colleagues used a flash mob study as a way to get an overview of a topic on a larger scale. In a large, qualitative flash mob study on what matters to patients after hospital admission, it was discovered that fewer data were missing due to the quick and easy approach (as much is not asked of participants, they rarely skip a question) (van den Ende et al., 2021). Therefore, the research question was answered in a better and more reliable way.
The flash mob is situated in practice, allowing for direct contact with and feedback from the community. Where AR projects are often time- and resource-consuming, flash mob studies promise fast results (Schols et al., 2019). Additionally, the immediate outcomes from a flash mob study (within a few weeks after data collection) allow for a quick progression to a new iteration and next steps within the AR project. Lastly, as flash mob studies are more creative and fun, they can attract more attention and involve participants who do not usually take part in research (Moons, 2021). This aligns well with the fact that AR aims to benefit a community, not just involved individuals. Therefore, we consider flash mob studies to be very suitable for eHealth AR. However, to our knowledge, no studies have yet investigated the applicability of the flash mob as a method for AR eHealth projects.
This paper aims to investigate the applicability of flash mob studies for AR eHealth projects. We will do so by carrying out flash mob studies in different research project settings in the health domain, reflecting on our own activities, and drawing recommendations for others who want to use flash mob studies in AR.

Method
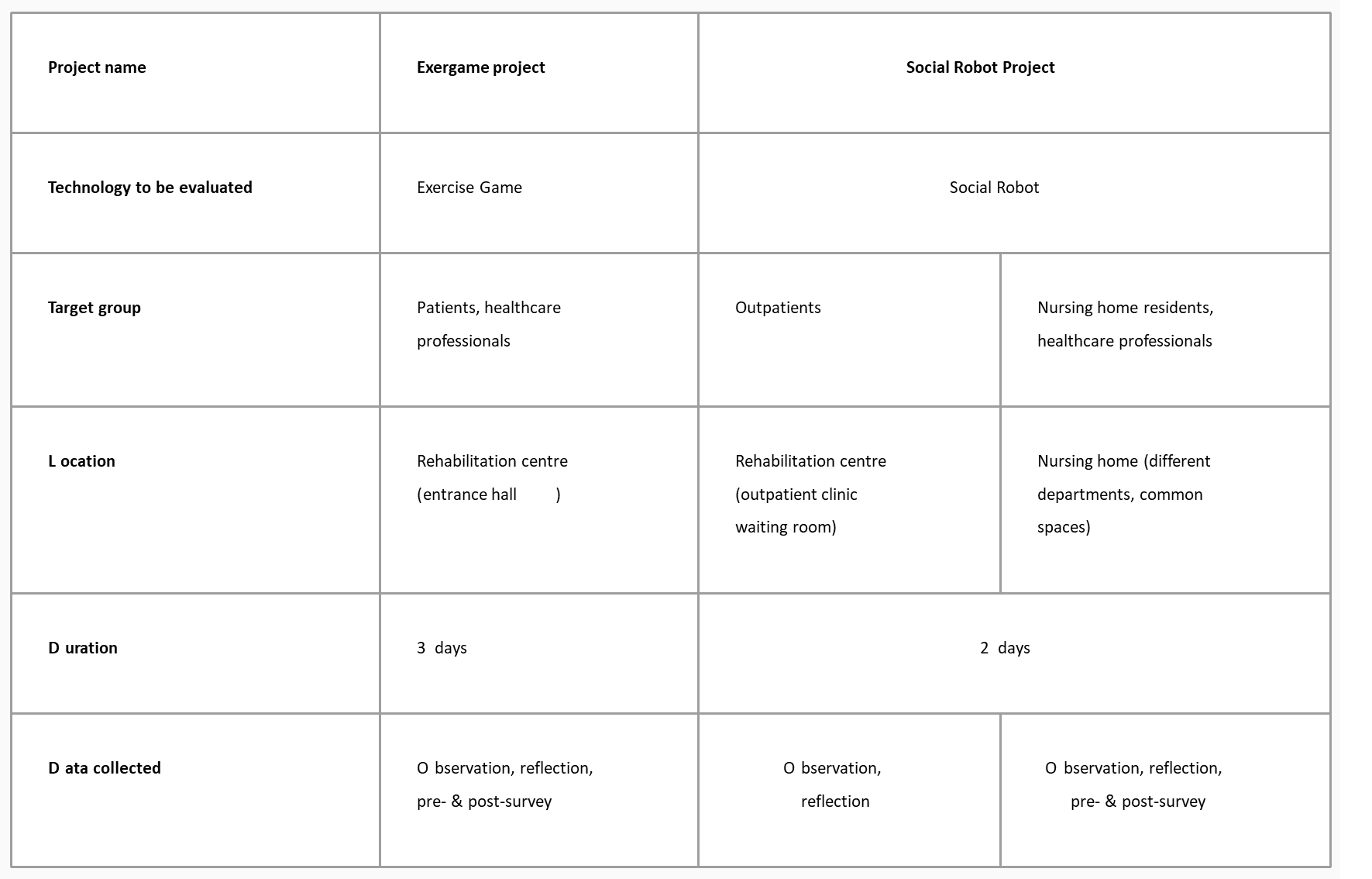
To investigate the applicability of the flash mob as a method for AR in eHealth projects, we conducted three flash mob studies, situated in two different research projects. While the content and structure of both projects differed, the data collection to evaluate the flash mob method was the same. Therefore, a short introduction of both research projects will first be given, followed by a combined data collection and analysis section. An overview of all three flash mobs can be found in Figure 1. While both research projects had elements of AR (e.g., making a change in practice), the projects were not specifically set up as AR. However, for our analysis, we use AR as a framework and relate our findings to the key elements of AR (cycles of planning, action, and reflection; research in practice; stakeholders as co-researchers; and scientific as well as practical knowledge).
Exergame Project
The first flash mob that we conducted was part of an Active Assisted Living (AAL) Exergame project. Within this participatory research project, an eHealth program that offers exercise games was developed and evaluated at a rehabilitation center. The flash mob study was conducted as part of the evaluation of the developed program. For the flash mob, a large television screen (approximately 1 by 2 meters) was set up in the entrance hall and both patients and healthcare professionals could walk by, try out the system, and fill in a short survey about their perception of the exercise game. The TV screen was on at all times during the study, displaying the start screen of the program to draw attention. The participant survey included an informed consent form that must be completed before participants could answer the other questions. The answers to this survey (i.e., the data collected through the flash mob method) are not used or presented in this paper, as we focus on the method and process itself. The study was set up together with the innovation manager at the rehabilitation center, who not only helped with practical matters within the center (e.g., setting up technology) but also provided input and feedback on the study set-up and survey questions. Participants could spontaneously join the flash mob, but to make healthcare professionals aware that the study would take place, a message was put on the internal digital bulletin board a week before the study began.
Social Robot
The second eHealth research project in which we applied the flash mob method was the Social Robot project, which aimed to evaluate the use of a social robot in rehabilitation and nursing care. In the project, new features were developed for a social robot, which were tested and evaluated via the flash mob method. Within the Social Robot project, two different flash mobs were conducted, which focused on the evaluation of a social robot in a healthcare setting. The first flash mob took place in the waiting room of the outpatient clinic at the same rehabilitation center that participated in the Exergame project. The setup included the social robot and a laptop to fill in the survey. In this flash mob, patients briefly interacted with the social robot before and after their appointment (e.g., answering questions about their appointment), and finally filled in a short questionnaire about their experience with the robot after providing informed consent at the start of the survey. Again, these content-related answers are not included in this paper as we only focus on the flash mob as a method. As in the Exergame flash mob, a message was posted on the bulletin board to inform staff ahead of time. In the second flash mob, at different departments of a nursing home, both patients and healthcare professionals interacted with the robot (e.g., playing games) and filled in the same questionnaire. Like in the Exergame project, the studies were set up together with employees from the two healthcare organizations who helped plan the flash mobs. In this flash mob, a schedule was created for when the robot would visit each department. The schedule was communicated with the healthcare staff internally.
Data Collection and Analysis
Two types of data were collected. First, a pre- and post-study survey were conducted to assess the perceived usefulness of the flash mob among the organizing partners. The surveys were sent via email, to the different contact persons at the participating organizations. Both surveys started with information about the research and participants had to provide their informed consent before continuing. In the pre-survey, next to some demographic questions, participants were asked about: 1) their expectations for the flash mob; 2) what they consider as a successful flash mob; and 3) whether they had any other remarks or questions. In the post-study survey, we asked participants: 1) how they experienced the flash mob; 2) whether they saw this as a useful way of doing research and why or why not; 3) whether the results were as they had expected and why or why not; 4) what they would do differently in a future flash mob; and 5) if they saw more opportunities to apply the flash mob method in their organization. The answers from the pre- and post-survey were thematically coded by the first author.
The second type of data collected was observations made by the researcher who was on site most of the time, and a reflection on these observations together with the co-authors after each flash mob. These were observations of passersby who did not provide informed consent to participate in the study. However, when we noticed somebody looking at our study set-up, we orally explained that we were performing a test of the technology, and of the flash mob method. When people then commented, for example, their opinion about doing a study in the entrance hall of the center, we informed them in the conversation that this was also interesting for us to hear about. We did not take any notes about these passersby except an aggregated summary of the general sentiment of all bystanders towards the flash mob in our field notes. This made it possible for us to reflect on the method and how it is perceived while respecting their anonymity.
The notes mainly recorded what did not go well, what we noticed, and what comments we received from participants. The notes and reflections of the researchers were organized into themes. We discussed these outcomes and reflected on them especially in relation to the key elements of AR, but also to plan the next flash mobs within this study and potentially in the future. The reflections were done in conversation between the authors as well as individually by the first author who was present at all flash mobs. We generally think that reflection, and sharing the lessons learned from these reflections, are crucial to (participatory) research. Since the survey results represent the perception and opinion of the participating healthcare institutions and the observations reflect the researchers’ perception of the flash mob, the results are presented separately, but combined conclusions will be drawn based on both outcomes.
Results
Based on the researchers’ observation notes, we identified four themes concerning the applicability of the flash mob method for AR eHealth projects: 1) initial hesitation; 2) interactions outside of the study; 3) help of insiders; and 4) purpose of the location. These themes are described in more detail below. The description of results from the pre- and post-survey, which represent the perspective of participating healthcare institutions, were analyzed separately and are presented after the themes.
Initial Hesitation and Expectations
During the three-day Exergame flash mob, there were five participants on the first day, eight on the second, and 13 on the last day. According to the organizer from the rehabilitation center, this was unrelated to the day of the week, since they had actually expected the second day to be the busiest. Thus, it seems that people needed some time after first seeing the flash mob set-up before they eventually got involved. Some participants explicitly expressed this initial hesitation, saying that after seeing the flash mob while walking by a few times they got curious and wanted to know more. Finally, some individuals expected us to be there the whole week instead of only three days, or said that they would come back tomorrow on the last day of the study.
Interactions Outside of the Study
In the Exergame project flash mob study we observed interactions, questions, and attention from people who did not participate (both patients and employees). Some were interested but had no time to participate while others had questions about the eHealth program that was being tested but felt that it was not for them. There were also relatives and non-medical employees whose attention was drawn due to the unusual location of the flash mob. Therefore, from the first Social Robot flash mob on, we explicitly started to count interactions and made notes of remarks outside of the study questionnaire to gain insight into these additional interactions. In the two Social Robot flash mobs, part of the interaction with the social robot consisted of filling in a survey on the tablet of the robot. Some participants only completed this activity but were not willing to fill in the questionnaire about their experience with the social robot.
Help of Insiders
In the Exergame project flash mob, a healthcare professional who participated in the study early on offered to send an email to his colleagues asking them to participate as well. Several participants later stated that they had already seen or been interested in the flash mob but only decided to participate after the message from their colleague. There had been an announcement via the internal communication of the rehabilitation center, but seemingly this had not had the same effect. Similarly, in the second Social Robot flash mob at the nursing home, some healthcare professionals were interested in the social robot and, after participating themselves, motivated patients and other healthcare professionals to take part as well by calling them over. We noticed that they only invited specific participants (e.g., saying, “This is something for you”), and did not push when an invitation was declined. While the researchers involved in the different flash mobs invited participants, the snowballing started by these insider participants reached people in a different way and drew more attention to the flash mob.
Purpose of the Location
The three flash mob studies were conducted in different locations, serving different purposes (e.g., waiting room, living room, restaurant). The Exergame project flash mob took place in the entrance hall of the rehabilitation center, which also served as the waiting room for the occupational therapists and as an extension of the restaurant during lunch break. The first Social Robot flash mob was conducted in the waiting room of the outpatient clinic at the rehabilitation center, while in the second Social Robot flash mob, the robot was brought to different departments of the nursing home. There, the flash mob usually took place in the communal space or living rooms of the departments and during the lunch break the social robot was taken to the canteen. When people came across the first two flash mobs, they sometimes did not have the time to participate as they were headed somewhere or waiting for an appointment. We tried to make it possible to participate during the waiting time, but this did not always work out as some time was needed to familiarize themselves with the technology and to fill in the survey. Lack of time was less of a problem in the Social Robot flash mob where the robot was brought into the communal spaces where residents and healthcare professionals were spending time together. Further, the different locations also attracted different types of participants. For example, the entrance hall was open to everyone and a lot of people walked by, whereas the outpatient clinic waiting room was mainly populated by patients waiting for their appointment.
Pre-Survey
To include not only the researchers’ perspective but evaluate how participating organizations perceived the flash mob, a short pre-survey was sent to the innovation manager at the organizing party in the Exergame project flash mob and to two health technology advisors and a nurse in the Social Robot flash mobs. In both studies, the main expectation of the participating organization was to gain insight into the usefulness and possibilities of the technology that was being tested. This was mostly mentioned in relation to the work of healthcare professionals, but in the Social Robot study, the usefulness for patients was mentioned as well. Some expectations differed between the studies. For the Exergame project, the organizing institute was not only interested in the technology that was being tested but also wanted to learn about the usefulness of a flash mob study as a way of testing technology in practice. One of the participants from an organizing party in the Social Robot flash mob said the “research can lead to possible inspiration in employees.”
Additionally, participants were asked when they would see the flash mob as successful. In the case of the Exergame flash mob, having more than five participants was seen as a success. This related back to the expectations regarding the flash mob as a method, rather than the evaluation of the technology since the organizing institution had mentioned being interested in carrying out more flash mobs if the initial study demonstrated good outcomes. In the Social Robot flash mob, the main factor that made the flash mob a success was that it provided valuable insights to inform whether or not to implement, or further investigate, social robots.
There was also room for other comments or remarks at the end of the survey. Two participants in the Social Robot study added that they thought it was “very nice that the flash mob makes it possible to conduct this study at our location in an accessible way” and that they were “very curious.”
Post-Survey
The post-survey in the Exergame project flash mob was again completed by the innovation manager of the organizing institution. In the Social Robot flash mob, one of the health technology advisors completed the post-survey. When asked how they perceived the flash mob, both participants called it “nice,” and one added that it was an “open, transparent, spontaneous” method. Similarly, both stated that they perceived the study as useful, with one of them saying that it provided “nice insights.”
The outcomes in both studies were close to what the participants had expected beforehand. In both cases, the technology was not yet ready to be fully implemented, and there was some skepticism about the usefulness of the technology from healthcare professionals. For the Exergame study, “good attendance” was mentioned as part of the outcome.
When asked about things they would change in a future flash mob, only the participant from the Exergame study answered, saying that more shielding should be provided, as some patients felt awkward exercising in an open space where a lot of people passed by. Still, the same participant concluded that all eHealth innovations in their organization could be tested in this way.
Discussion
To evaluate the applicability of flash mob studies for action research and other participatory approaches in the healthcare and eHealth domain, we conducted three flash mobs and identified the following themes: 1) initial hesitation; 2) interactions outside of the study; 3) help of insiders; and 4) purpose of the location. Data from surveys with organizing institutions as well as observations from the researchers were reflected upon and combined in the discussion to provide lessons learned for others who wish to implement the flash mob method in their projects. After a discussion of these more general findings, we will go into more detail discussing the potential of flash mob studies in AR eHealth projects, and finally give recommendations for future flash mob studies.
General Findings
We conducted flash mob studies in two projects that examined if a certain technology could and should be implemented in practice. For this use case, we found the method to be valuable, as we were able to base the decisions on quickly gathered data from practice as well as opinions from larger numbers of participants than are usually involved in such short studies. Based on our experience, we also foresee a use to answer other (sub-)questions of a research project, like zooming in on aspects of a project that are still unclear, gauging attitude towards a project, testing the feasibility of ideas, and generally raising awareness for a project (as a by-product of the flash mob). However, there are aspects to consider when planning a flash mob, as we will outline in the following sections.
We observed that people are sometimes hesitant to take part in the flash mob study and that clear visibility of the flash mob in terms of timing, duration, and internal announcements within the whole organization is useful in overcoming hesitation, especially for healthcare professionals. Other types of announcements, for example via newsletters or information screens, might help to attract other participants, such as patients, as well. Kersting and colleagues (2022) mention that flash mob studies should be used for “popular and simple research topics” as these potentially attract more participants. However, their research targeted the general population, whereas for patient groups, research about their diagnosis could also be interesting. Therefore, future projects wishing to employ the flash mob should prepare a clear and suitable announcement strategy, including information on the aim, duration, and target group of the study. In practice, this could be as simple as having information posters near the location of the study.
In our study, the aim of the flash mobs was not only to gather data but also to reach out, involve, and inspire different stakeholders. As was also mentioned by the organizing healthcare institutions in the survey, giving attention to the subject of the flash mob (e.g., for a new eHealth technology, or general innovation policy) is an important goal that the flash mob can also fulfill. However, to our knowledge, previous flash mob studies in healthcare focused on the collection of large quantities of medical data, and outreach was a side effect at most, as it is expected that studies that draw attention also draw more participants (Moons, 2021). In our second flash mob, we started to track the number of interactions and made notes of comments or questions that we received unobtrusively. It was important to us that our tracking of the outreach would not put an extra burden on participants, nor go against the idea that a flash mob should collect very limited data as “the research question can be answered with a small data set per patient” (Schols et al., 2019). In future flash mob studies, we plan to continue using similar unobtrusive ways of tracking the outreach.
We as researchers were an outside party to each flash mob and therefore not familiar to the healthcare professionals or patients. What really helped us, especially in the first and, to some extent, the third flash mob, were the efforts of insiders to convince others to participate. All of the healthcare professionals who reached out to others were enthusiastic and motivated to drive the research, characteristics which are often attributed to ‘champions’ (stakeholders from within an organization who drive a project from an intrinsic interest, going further than what is their job) (Greenhalgh et al., 2004; Hendy & Barlow, 2012). In both of our studies, these champions became involved during the conduction of the study, although it would have been ideal to know and involve them earlier on. Involving champions and other motivated stakeholders — for example, encouraging and inviting participants — also aligns with the principles of AR, where stakeholders become co-researchers (Reason & Bradbury, 2007). However, it could be argued that recruitment via champions poses ethical issues, as some might be convinced to participate out of obligation to the champion. In our case, the champions were healthcare professionals who either recruited colleagues or patients. They only did so after completing the study themselves. As the champions only asked others to participate but did not push further once declined, we believe that their involvement in our studies can be evaluated positively, but future studies should be mindful of forced participation or unethical behaviors.
We also found that the location in which a flash mob takes place can influence if and how people participate. For example, during the Exergame flash mob, some participants were hesitant to try the system while others in the entrance area could see them. Therefore, there are some variables to consider when choosing a location. First, think about the target group and their relation to the location. This can include questions like whether the target group actually comes to this location and whether they have the time to participate in a study while they are there (e.g., patients in a waiting room might have five to ten minutes if they come a bit early, but usually not much more). Similar considerations apply to locations that serve a purpose but might still work as a flash mob location. An example that we also experienced in our study is an institution’s canteen or restaurant. While patients and healthcare professionals come there with different purposes, they might be able to make time for the study.
Another consideration is the fact that flash mob studies need to take place in open, visible spaces, as opposed to closed-off lab settings. In our opinion, this holds advantages (reaching different audiences, more attention for the study) as well as disadvantages (feeling ashamed of participation, privacy concerns), and researchers need to weigh these considerations for each study. Particularly in studies where participants are asked to perform a task that involves the use of technology, they might feel awkward when others are (potentially) watching them. The importance of participants feeling comfortable at the research location has been emphasized before (Fox et al., 2021), and we suggest this should be the primary consideration for studies that require actions from the participants. Additionally, in public locations, people other than those being targeted might be present, ask questions, and even want to participate. Researchers should determine a strategy for dealing with such requests beforehand. In future projects, we are considering a separate way for non-target group members to offer opinions and feedback (for example, a notice board where they can place post-it notes). While it can be informative to have conversations with bystanders, this should not distract from the main aim of the study.
As the data we collected in the flash mob studies was not extensive, it was decided to leave the analysis to the involved researchers. However, in our reporting and dissemination efforts, we included the involved institutions and worked to make our findings understandable and usable for them. We produced fact sheets of the study outcomes, the rehabilitation center prepared two vlogs (one for the Exergame flash mob and one for the first Social Robot flash mob) which they shared on social media, and we wrote a blog post that informally explained some of our recommendations for future flash mob studies. A key element of flash mob research is the quick analysis and reporting of results. However, in AR, stakeholders become co-researchers and should be involved in the analysis and reporting. This means that they need to make time not only for the conduction of the study but also for data analysis. For some stakeholders, like healthcare professionals, this can be challenging. Additionally, stakeholders might need additional training to analyze data. A more accessible way could be to have focus group discussions with the researchers and stakeholders where the data is presented and discussed to make meaning of it with the stakeholders.
A limitation of our study is that the flash mob studies in both research projects were driven by the involved healthcare institutions and researchers. Patients were not consulted in the planning of the studies but only took part as participants. This decision was due to the limited time frame in both projects, as the studies took place in the last months of the project run times. This time constraint made the flash mob, with its fast-paced data collection, analysis, and reporting, an ideal method.
Linking eHealth AR and the Flash Mob Method
To discuss the applicability of the flash mob method for eHealth AR, we will highlight several elements of AR and flash mob studies and the connection between them: 1) AR being situated in a community; 2) AR actively involving various stakeholders; 3) flash mob studies being very fast-paced; and 4) flash mob studies involving large groups of people. Furthermore, we will explain how one of the challenges of flash mob studies that we mentioned earlier, namely the involvement of champions, is mitigated in AR. Throughout this section, we describe for which research questions, which stakeholders, and at which stage of an eHealth AR project flash mob studies hold potential.
A key element of AR is the fact that the research takes place in a community instead of a lab setting. While situating research in practice is a good first step, to make such a change last it is important to involve community leaders, such as local government organizations (James & Buffel, 2022). A flash mob study makes the changes brought about in a project very visible and can be used as a showcase to convince local leaders. Additionally, drawing (media) attention emphasizes the outreach and importance of a project, which might convince local government. In our opinion, flash mob studies to support AR in practice work best for communities that have a clear (meeting) space, for example, community centers. Of course, the previously mentioned considerations about how suitable a location is for the given flash mob still apply.
In eHealth research in general, but also participatory approaches like AR, those with a higher education level are more likely to participate (James & Buffel, 2022). Furthermore, the decision of who gets to participate frequently lies with the researcher (Vines et al., 2013), and might be based on previous collaborations (Hand et al., 2019). This leads to a biased, select group of participating stakeholders. Flash mob studies can serve as a way of lowering the barrier to participation. By making research participation fun, engaging, and spontaneous, people who might usually be reluctant or uninterested in research projects can easily get involved. In the Exergame case, for example, patients could join without a referral from their therapist, who might make mistaken assumptions about whether or not somebody is able to use a technology and wants to participate (Wilderink et al., 2021). Our assumption is that flash mob studies can best support those AR projects (and sub-studies) where no previous knowledge or (digital) skills are required for participation, to allow for a very low barrier and involve those without affinity to research.
Flash mob studies are meant to be carried out very quickly. This not only includes short periods of data collection but also quick analysis and feedback of outcomes to the involved parties. In our experience, this worked very well. When everybody involved is aware of the fact that the analysis and reporting need to happen quickly, they can schedule time for this. It is not uncommon for AR processes to take a lot of time (Grant et al., 2008). In our opinion, flash mob studies could be implemented to speed up cycles and help make quick decisions. While we examined whether or not to adopt a new eHealth technology or device, this could apply to situations where short input from large groups is more valuable than thorough conversations with a smaller group. However, we generally believe that the outcomes of a flash mob are more than a “quick and dirty” approach. The study was quick, but the results were still somewhat detailed, and useful to answer the questions, making it “not dirty” in our opinion.
Another central point of flash mob studies is that large groups of participants can be involved. This is possible even in such a short period of time because the burden for participants, and the time required from them, are kept to a minimum. A problem of AR is not only that the process itself takes a lot of time, but because of that, participation in AR also becomes very time-consuming for stakeholders (Grant et al., 2008). We believe that flash mob studies can make research more accessible also for those groups for whom longer-term involvement could be a burden. This can also be an easy, low-threshold way of getting the target group in contact with a research project or with an eHealth technology still under development, which can be interesting at the start of project phases.
A problem that we noticed in the way we carried out our flash mobs was that we had little involvement of “champions” on the work floor. The innovation managers and technology advisors we worked with helped set up and promote the flash mob, but peer contact (e.g., between physical therapists) worked much better for promotion. However, we expect this to be less of a problem in AR projects, where there is already good contact with some healthcare professionals, as they are likely involved as co-researchers. In our opinion, AR and flash mob studies supplement each other well in projects that already have some involvement from the work floor but wish to receive additional input from peers.
Recommendations for Future Flash Mob Studies
From our study, we can conclude that flash mob studies are a potentially suitable method for eHealth AR projects. For setting up a flash mob study we suggest the following recommendations:
-
Find “champions” from inside the organization who can encourage peers to participate.
-
Make people aware of the flash mob beforehand, for example through internal communication channels. This way, spontaneous participation is not excluded, but those who need to consider participation have the time to do so.
-
Similarly, have materials present during the flash mob to inform and attract the attention of potential participants.
If general outreach is one of the goals, think about how to track that. This could include the number of interactions (regardless of eventual participation), or questions and comments received.
-
Consider what location is most suitable for your flash mob. Consider aspects like accessibility, visibility, and activities associated with the location.
Conclusion
In conclusion, the flash mob holds a lot of potential for AR eHealth projects, as it is naturally situated in a practical setting, which also makes it easy to involve relevant stakeholders, even those who might not usually join a research project. The fast pace of the flash mob is suitable to speed up the often-lengthy cycles in AR. However, as the method is relatively new, and has not been used in studies comparable to ours, there is still a lot to learn. For example, it would be interesting to study the effect of different locations, and promotion strategies, on participation in flash mob studies. Based on our lessons learned, we were already able to make some general recommendations, namely: 1) promoting the flash mob through suitable channels ahead of time; 2) tracking interactions, questions, and remarks aside from the study; 3) finding a suitable location for the study; and 4) involving insider champions to facilitate participation.
Acknowledgements
The authors thank Roessingh, Centre for Rehabilitation, Enschede, and Zorggroep Sint Maarten, Oldenzaal (both in the Netherlands) for conducting the flash mobs with us in their facilities. We also thank all those who participated in, or engaged with, the flash mob studies at the different locations. Lastly, we want to thank Dr. Marian Hurmuz and Isa Kottink for their help in conducting the flash mob studies.
Part of this study was conducted within Active Assisted Living (AAL) project SALSA (project no: 2018-5-46-CP). This study was also partially supported by the Scotty project (DIH-HERO technology transfer experiment), funded by EU’s Horizon 2020 research and innovation program (no: 825003).