


Global health research addresses large-scale health issues worldwide, often focusing on marginalized, impoverished, and vulnerable populations. Participatory research in global health provides a practical and ethical approach to working toward positive health change while respecting a community’s autonomy, desire for change or intervention, embedded systems of communication, and social norms (Sawaya et al., 2018). Intervening to address social norms around an entrenched health problem has been identified as a primary driver of effective behavior and social change. Conversely, regulatory interventions often have very little impact on changing behaviors as part of persistent cultural norms (Cislaghi et al., 2019).
Participatory approaches and methodologies serve overarching research values of working with research participants and honoring community knowledge while utilizing specific research tools and methods that both engage the community to discuss difficult and stigmatizing health issues and encourage community-centered behavior and social change. Participatory approaches such as community-based participatory research (CPBR) and participatory action research (PAR) are increasingly recognized and encouraged in global health work by multinational donors, researchers, and practitioners (Wallerstein et al., 2017). However, there is a gap in research-based evidence that evaluates whether participatory interventions using a social norms research approach have the intended impact (Sood, Kostizak, & Stevens, 2020).
This paper explores two visual tools — social network mapping and 2x2 tables — used for participatory data collection in interventions that seek to shift social norms to facilitate change for women’s health. We begin with an introduction to social norms as the context in which participatory approaches and tools can be used to effect change. We then outline two examples of research to discuss how social network mapping and 2x2 tables were used as part of participatory methodology in public health interventions that tackle social norms. We conclude by identifying these tools’ limitations and challenges as well as their potential for application to other research areas. This paper seeks to answer the following questions: How have the visually informed participatory research tools, social network mapping and 2x2 tables, been used to promote social and behavior change? How can these participatory mixed-method approaches support the development of programs, monitoring and evaluation (M&E), and assess social and behavior change for public health issues around the world?
Social Norm Theorizing
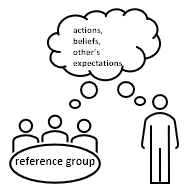
Social norms are the unwritten rules that guide human behavior: they are what we do, what we believe others do, and what we believe others think we should do (WHO, 2010). For their existence, social norms require a reference group, i.e., a network of people to whom we identify and compare ourselves (Lapinski & Rimal, 2005). This reference group determines norms because identifying a behavior with a specific group influences whether that behavior is considered normative within the group and, in turn, may predict whether a new behavior will be adopted (Goldstein et al., 2008). Members of a group expect, are expected to follow, and are motivated to follow norms because of sanctions for non-adherence and rewards for adherence. Finally, collective norms are what people actually do, i.e., the actual prevalence of a behavior. See Table 1 for these distinctions in social norms constructs.
Change of social norms requires cognitive shifts in deeply embedded schema and scripts formed within dynamic interpersonal relationships with people who serve as primary reference groups. Social and behavior change communication theory states that social networks are primary mechanisms that may drive behavior change through the action of education and dialogue (communicated messages) that counteracts prevailing ideas about a given area of concern. There are many behavior-change theories that operationalize social norms and target types of norms. For purposes of this discussion, social norms are the construct that we mean to change via public health interventions by using participatory methods such as social network maps and 2x2 Tables. The inclusion of audience participation makes these tools effective for applying to social norms change with deeply embedded cultural practices where the potential social consequences for engaging or not engaging in the practice seem dire and structural barriers seem great.

Research Examples
This paper discusses the application of social network mapping and 2x2 tables to social norms around the issues of female genital mutilation (FGM) and menstrual hygiene management (MHM). After briefly introducing the context of these issues and our work, we will introduce each tool, how to use them, and provide examples of how they were used in our work, including their advantages and limitations. Two illustrations of participatory research with young women and relevant community members to address global health concerns will be used to show how these participatory visual tools have addressed health-related social norms in low-income countries. These examples come from our work on significant women’s health issues as sponsored by the United Nations under a framework that addresses women’s and girls’ health as part of the global Sustainable Development Goals (UNFPA/UNICEF, 2020). Small focus group discussions and evaluations were part of the framework for participant involvement in both the FGM and MHM programs. Consultation with global and local experts, and discussion with program implementers, followed by rigorous pretesting of each of the tools were all used to ensure that these methods were acceptable.
Research and Programs to Impact Female Genital Mutilation
A framework was designed to provide adaptable yet standardized participatory measures of social and behavior change for female genital mutilation (FGM) in Ethiopia and Guinea (Sood, Kostizak, Lapsansky, et al., 2020). Called ACT, the framework addresses: “A” assessing for affective and normative data about the practice; “C” the context in which these practices occur; and “T”, tracking or monitoring of behavior change (Sood, Kostizak, Lapsansky, et al., 2020). FGM is the practice of altering, injuring, or “cutting” female genitalia for non-medical purposes and is an international public health concern affecting millions of girls and women worldwide (UNFPA/UNICEF, 2020). Practiced in cultures in more than 30 countries throughout Africa, parts of Asia, and the Middle East FGM now exists in nearly every country due to migration. It is tied to social norms of marriageability, perceived purity, and social acceptability of girls and women across the lifespan. Yet, it results in trauma, chronic pain, severe complications with sex and childbirth, and even death from infections or blood loss.
Research and Programming to Impact Menstrual Hygiene Management in India
The Girls’ Adolescent and Reproductive Rights (GARIMA) program addressed menstrual health and hygiene management (MHM) in India (NRMC & Dornsife School of Public Health of Drexel University, 2018). Unsanitary practices of MHM lead to poor hygiene, infection, disease, shame, and social ostracization of menstruating females (Sinha & Paul, 2018). Addressing menstrual hygiene management in India is a critical area of women’s health spotlighted by UNICEF to address gender equity and economic policy in the Global South (Sommer et al., 2021). Inadequate MHM leaves girls and women vulnerable to disease and is a primary driver of gender inequality and social exclusion (NRMC & Dornsife, 2018). A culture of silence has been identified as the root of poor MHM, leaving young girls with poor knowledge and myths related to the care of their bodies during menstruation. While infrastructure around adequate facilities for washing and disposing of menstrual products is part of the solution, influencing social networks of the young girls has been found to have a greater impact on behavior change, including addressing larger sexual and reproductive health issues in India (NRMC & Dornsife School of Public Health of Drexel University, 2018; Sinha & Paul, 2018; Sommer et al., 2021).
Methods
Ethics and Positionality Statements
This research was approved by Drexel’s IRB as well as a local IRB and it further followed UNEG (United Nations Evaluation Group) standards and ethical guidelines. Funding and programming for this research were provided by UNICEF. Researchers first gained oral consent from participants. Consent forms were translated into local dialects, though verbal consent was given as customary with populations where literacy may be low and local dialects may not be translated. Postcards were left with participants to provide research information and follow-up contact information. Standard protocols were followed regarding global health research and consent, ethics, and respect for personal autonomy (Sawaya et al., 2018).
The research reflected in this paper was designed by Dr. Sood through the Dornsife School of Public Health in partnership with UNICEF. Local researchers and practitioners collected, cleaned, and transcribed the data. J.R. HaileSelasse is a doctoral research fellow working with Dr. Sood at the Dornsife School’s Community Health and Prevention while the other two authors are researchers at Drexel University in Creative Arts Therapies, College of Nursing and Health Professions. Both Dr. Sood and Dr. Kaimal are of Indian descent with contemporary ties to that country while HaileSelasse and K. Snyder are white Americans. All four women share a worldview that includes the promotion of women’s health and human rights, respect for the agency of participants in research, a pragmatic focus on working toward positive change in people’s lives through research, program implementation, evaluation and monitoring, and community-engaged learning whenever possible. Our case study examples are from research conducted by Dr. Sood’s team with community teams in the field in each location. It is our hope, as a cross-disciplinary team, to share the value of these participatory visual tools and community-engaged methodology.
Social Network Mapping
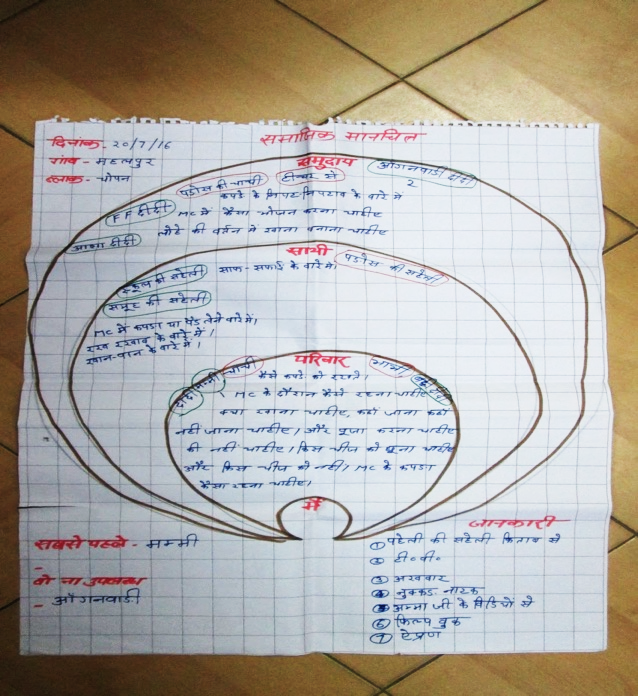
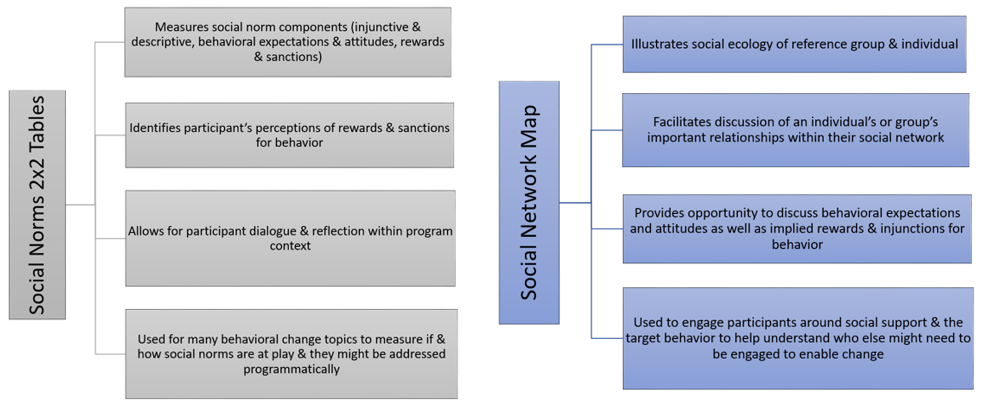
Social network mapping (SNM) is a visual technique that illustrates how community members are connected and how information flows through social networks (Scott, 2000). Participants draw or fill in graphics or “maps” that show and list who is in their social network in relation to themselves and others. This illustrates where and how information is shared and can even be used to explore types of information (Scott, 2000). As such, social network mapping is a great way to identify participants’ key sources of information as well as barriers to communication. This tool is based on social network theory, which explains decision-making as largely influenced by group relationships, norms, and expectations (Ulin et al., 2005). When a participant completes a map, not only does it provide data on the nature of their social network but also offers insight into how they see or perceive that network and their role within it. As a transformative activity, SNM can have a therapeutic effect on participants, where they visualize themselves, perhaps for the first time, as part of a social network and within the context of the health issue being discussed. With this information, researchers can assess the influence of structural and relational dynamics on health status (Luke & Harris, 2007). The maps themselves can take many forms (Figure 2). For example, they may show concentric circles with each one representing different layers of society (e.g., family, peers, community). Participants can also draw maps with themselves in the middle and their contacts connected by lines, like a web. The size of the map components can be used to illustrate the importance of that person within a social network with larger circles, lines, or arrows (web pattern) indicating greater importance. No matter the format, the key is to have maps that illustrate relational ties. Each format may have its own potential benefits for data collection, illustration, and transformation.

This preliminary exercise with the participant helps show who within the social network influences their beliefs and behaviors. By identifying such network groups within an ecological model, the participant is primed to consider the way that they have come to view a social norm, practice, or expectation. Participants can then visually map individuals whom they consider as providing accurate information as well as people who need to be included in future programming. Then, the community-based program efforts focus on reaching the individuals identified as important by the participants. Ongoing programs then target such beliefs and support social network changes. For example, primary caregivers may be brought in for dialogue or other activities to engage them in considering alternatives to the detrimental practice.
In later research stages, diagrams might be re-examined to monitor the impact of community interventions, including quantification of changes in patterns of interpersonal communication among program participants. This provides programmatic visual proof of any intended expanding networks that have effectively displaced the culture of silence around these issues. When it comes to program evaluations, maps can be specific to show whom participants speak with about the program. By conducting another SNM later in the program, participants may develop personal insight into changing views about the detrimental practices and new health practices as well as continued social norms and networks that either support positive change or inhibit it. This information equips field experts to quickly address the community in new ways to bring about desired change, developing programs that fully support all community members. Beyond research and evaluation, social network maps encourage participant and community dialogue, and, as seen in later case examples, helped the girls who participated in our study to identify whom their community-based programs needed to work with and how. Allies are leveraged for promoting desired behaviors while individuals who create barriers are assessed for additional interventions to promote behavioral change.
How to Create a Social Network Map
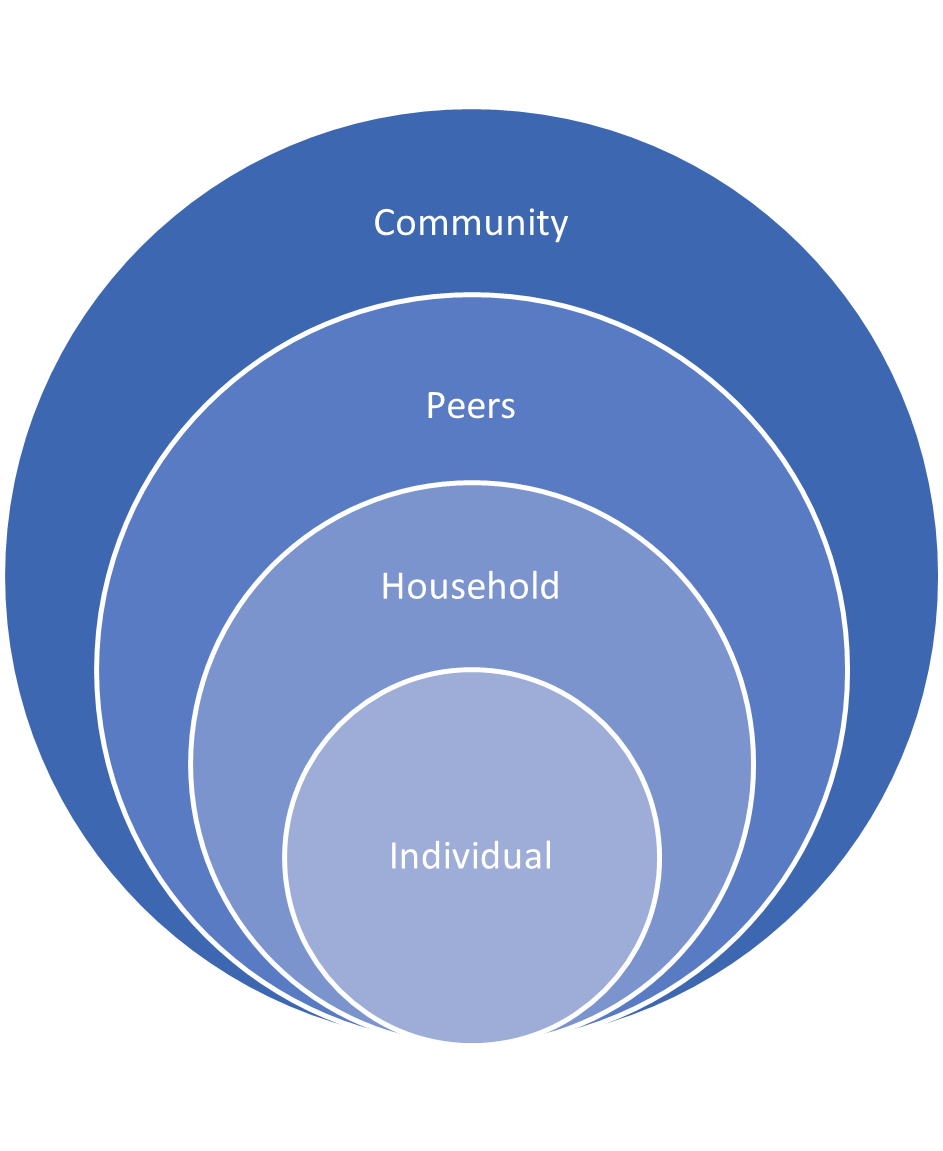
The activity of mapping begins with a visual template, as seen in Figure 3, that is either printed and handed to the participant or drawn during the process as participants speak. The mapping process translates well to low-technology environments and could be done on blackboards with photos taken of the process and final product. Face-to-face settings can use paper, flip charts, or other simple means to create maps. Web-based, sharable graphic applications can be used in virtual settings. In any setting and use of material, providing an introductory example to participants is a good means of building participant confidence as well as maintaining the continuity and integrity of the data. Participants are asked to identify the people in their lives and their places within each of the categories of social influence, along with provided examples. As they list individuals within each category, participants are asked to identify what types of support they have received from each person. Researchers/facilitators should make notes about these relationships, including relevant themes such as allyship, barriers, and any foreseen potential barriers to positive change with the intervention. The participant is then asked to rank the people that they have listed in order of support and influence. Other probes that can be part of the process include asking a participant to consider their level of investment in each relationship in the context of the targeted health issue. Filling in this social network map illustrates social and informational concepts about the health concern and environmental influences. This will be important for data interpretation and analysis to assess the social norms relevant to the health concern.

One advantage of social network mapping is that resulting data may be interpreted relatively quickly and in the field. Data are first divided based on participant characteristics such as gender, age, socio-economic status, and either change of time or intervention versus comparison if used at the M&E phase. Frequency counts are tallied across all observations and different social categories, noting the most common level of social influence. This can include counting allies and barriers to behavioral change as relevant to findings. Finally, thematic analysis helps to pull out the most common themes and ideas that explain how individuals in this group perceive their social network influence in relation to the health concern.
Reviewing the data and relevant themes provides insight into the importance of engaging different reference groups in the community. Aggregate data reveals the most important community members’ influence over a particular health behavior to target programs and interventions. Responses to any probing questions used may also suggest how communication flows with the various reference group members.
2x2 Tables
The visual participatory 2x2 tables method aids researchers, participants, and communities in assessing the existence, persistence, and change in social norms over time. Though they can be simple visual depictions with limited text and four boxes, conceptually they are complex and require consistent high-quality training for researchers/facilitators. Pretesting is strongly recommended. The facilitator of this activity needs to have a clear understanding of the types of social norms that it measures. The exercise must be understood as designed to measure three types of social norms as discussed in the introduction and summarized here to emphasize the importance of training facilitators. The 2x2 Tables measure an individual’s behaviors or what we do, descriptive norms as what we think others do, and injunctive norms as what we think others expect or believe that we should do.
This tool provides rich mixed methods data for analysis that can be used to design programs, measure norms and behaviors at baseline and end-line, and measure change as part of monitoring and evaluating a program for efficacy. Resulting data includes frequencies and prevalence of behaviors and norms as well as qualitative data shared in discussions of why participants provide their answers and links to social rewards and punishments that are related to social norms. For these reasons, it is helpful to collect observational data and notes while the activity is underway. Importantly, the data allows programmers to understand if an issue is normative in nature. Generating the data allows participants to visualize differences between their approval, societal approval, social expectations, and behaviors. If facilitated, this leads to dialogue on why and how harmful practices persist due to normative and injunctive expectations. This data can also be used to revise the activity after pre-testing or to identify appropriate outcomes for a program.
How to Use a 2x2 Table
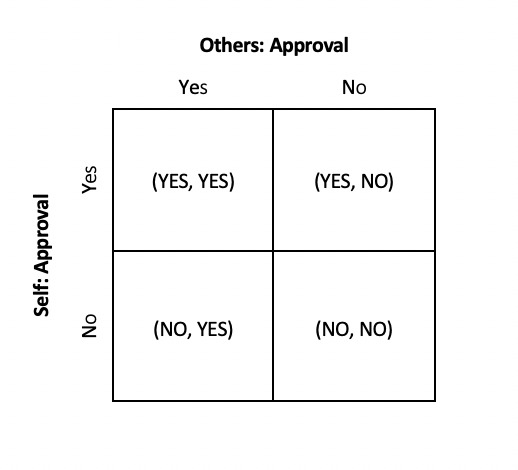
To conduct the exercise, clear definitions and examples of the target behavior should be provided, allowing participants to ask any questions or clarify what they are being asked to consider when filling in a table. Participants are first asked to identify, in their opinion, what proportion of community members engage in this behavior. This helps indicate their perceptions about the prevalence of a given behavior. Then they work through two 2x2 tables concerning a behavior. The first table measures attitudes by asking participants if they approve or disapprove of the behavior (Figure 4), and whether they think others approve or disapprove of the behavior. The second table measures injunctive and descriptive norms by asking whether others in their community practice the behavior and expect them to do so as well. The “others” in this case are members of the participant’s social network, comprised of individuals whose opinion matters to the participant as established by creating the social-ecological network map.
Participants are also asked to provide the associated rewards and punishments (Figure 5), which allows assessment of outcome expectancies. Any behavior can be measured using 2x2 Tables for Social Norms. It may be best to include 2x2 tables for social norms as part of a larger study so social norms can be compared to other factors like knowledge, attitudes, and behaviors. This allows the social and behavior change interventions to accurately target social norms as part of a comprehensive social and behavior change strategy.

To complete the two tables, participants need to respond to two separate questions with yes/no answers. The first questions are whether they approve of a given behavior, and to what extent they think “others” approve of a given behavior. Have them place a mark in one of the four quadrants based on their answers. If they answered yes to both questions, put a mark in the top left (yes, yes) quadrant. If they answered yes to the first question and no to the second question, put a mark in the top right (yes, no) quadrant. If they answered no to the first question and yes to the second question, put a mark in the bottom left (no, yes) quadrant. If they answered no to both questions, put a mark in the bottom right (no, no) quadrant. It’s important for the researcher to remind participants to respond only with yes or no answers. Emphasize while you understand that different types of people do and think different things, for this activity you want them to select either “yes” or “no” based on what they think more people do and think.
Next, have participants fill out the second 2x2 table for behavior. Use the same instructions as before. However, instead of approval, ask if “others” practice a given behavior and if they expect the participant to practice the behavior. Have them fill out Figure 4 in the same way as they did the previous table. If they answered yes to both questions above, put a mark in the top left (yes, yes) quadrant. If they answered yes to the first question and no to the second question, put a mark in the top right (yes, no) quadrant. If they answered no to the first question and yes to the second question, put a mark in the bottom left (no, yes) quadrant. If they answered no to both questions, put a mark in the bottom right (no, no) quadrant. Then, when helpful to the research and appropriate to the participant, ask them to reflect on the reasons why they are in a given quadrant to elucidate more context. Depending on the behavior in question, the first question on the second table can ask participants about their own behavior and the behavior of others. The table can then be followed by the question “Do others expect you to participate in this behavior?”
To ensure participants understand the activity, one can use several different representations. For example, ask each question and have them write the answers on a piece of paper, then read their responses aloud or pass them along to the interviewer (to maintain confidentiality). For non- or low-literate populations, one can use different colored stickers or sticky notes to display their answers. Once the responses are recorded, the interviewer asks a variety of probing questions depending on the behavior. For example, why they and/or others fit into the selected quadrants, discrepancies and/or concurrence between approval and behavior, and how individual- and societal-level change can be achieved to encourage participants to recognize and challenge social norms.
To analyze results from the 2x2 tables, data are pulled and divided into groups based on participant characteristics such as age, socio-economic status, etc. Frequency counts (content analysis) are made for each quadrant in each of the two 2x2 tables to look at both perceptions of the behavior (approval) and practices of the behavior for self and others. The frequencies for each quadrant help to understand how the participants feel in relation to injunctive and descriptive social norms (Figure 6); beliefs about the prevalence of behavior practices; beliefs about what others expect us to do; and social rewards or sanctions that maintain the behavior in question. Some quantitative analysis may be conducted to determine any significant differences by quadrant between respondent groups as well as within quadrants on approval/attitude and behavior tables. Thematic analysis helps to find common responses among the participants from the probing questions. Analyses may focus on statements related to rewards and sanctions for the continuation of the behavior, rewards, and sanctions for abandonment of the behavior, and other ways that the participant perceives the social expectations for the behavior.

Interpretation of the 2x2 tables consists of mapping frequencies of responses within the quadrants. When responses fall more heavily in the extreme quadrants (top left “yes/yes” or bottom right “no/no”) social norms are indicated as driving the behavior. Whereas when responses fall within the top right or bottom left quadrants, participants are assumed to either be abiding by a normative behavior that they would prefer not to practice or that they are challenging a widely accepted normative practice.
When using information gleaned from these tables, it is important to keep the context of the intended behavior change in mind. An intervention might promote the uptake of a new behavior such as using disposable menstrual pads, or it might promote abandoning an existing behavior such as FGM. When the data predominantly fall in the top left quadrant, this suggests that knowledge and awareness strategies are suited for intervention. Similarly, when responses fall predominantly in the bottom right quadrant, programs that ensure the maintenance of positive behaviors and support abandoning negative behaviors are indicated, since the behavior is normative. Additional program models may emerge out of the data looking at personal and environmental reasons, rewards, and punishments behind behaviors that may need increased communication interventions at different levels.
Results/Discussion
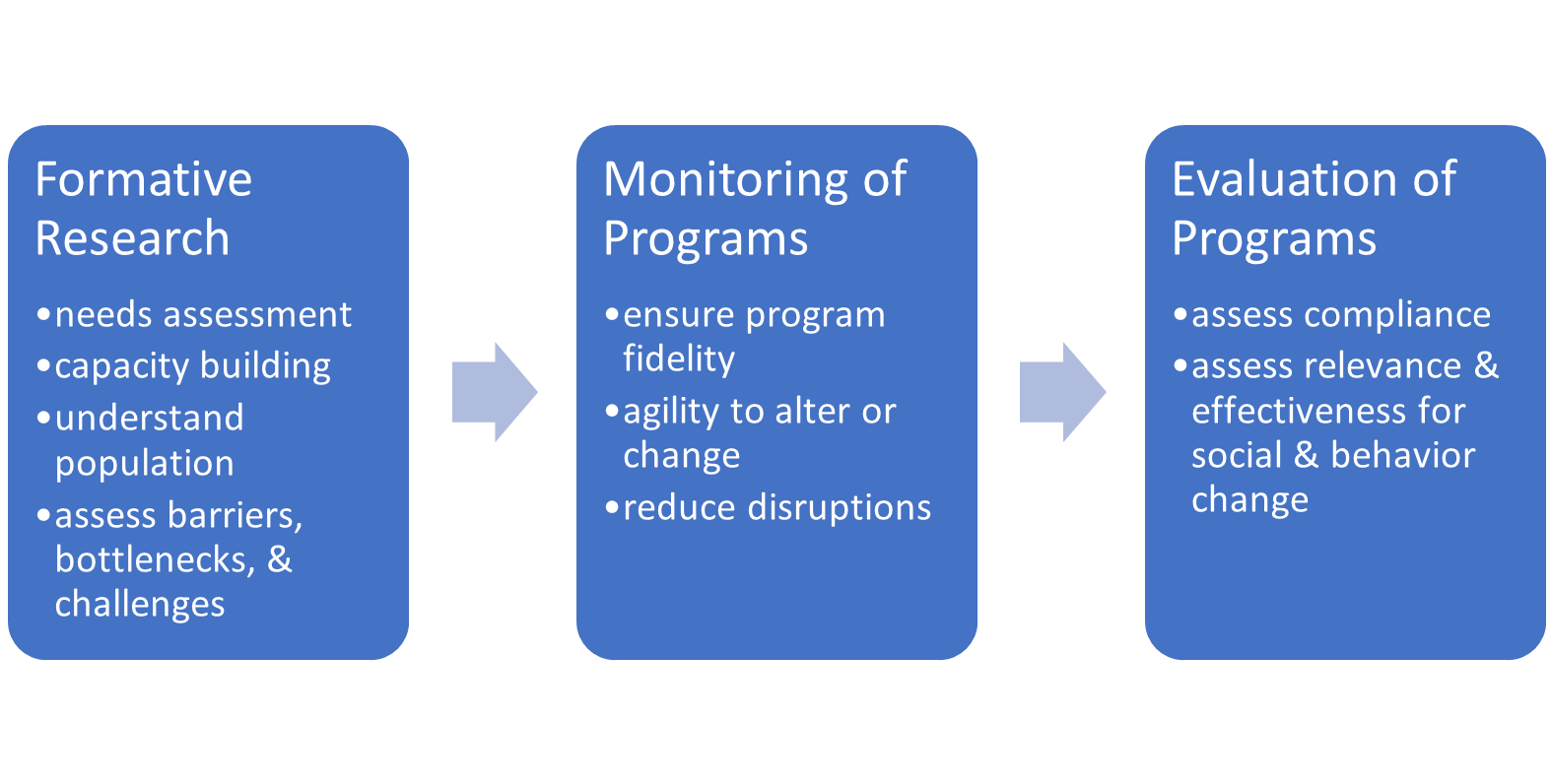
As part of ACT, participatory action tools are utilized to engage the target audiences in communities and to monitor program effectiveness to make changes in real time based on participation (Figure 7). These activities allow participants to reflect and discuss behaviors and norms and explore the reasons why these norms exist, especially when follow-up dialogue is facilitated as part of the activity. Social network maps and 2x2 tables were designed to be used together, with the latter exercise measuring norms by building off the former exercise that visualizes realms of social influence. However, these tools can be used separately or in conjunction with other relevant visual tools, participatory activities, and a range of quantitative and qualitative methods. When used together, it can be helpful to have completed maps visible as visual prompts to participants as they conduct the 2x2 table activity. For a step-by-step training and implementation guide for these visual tools, access the following link: https://www.unicef.org/documents/ act-framework-package-measuring-social-norms-around-female-genital-mutilation.

In Ethiopia, the use of the 2x2 tables helped researchers and frontline community program workers to parse participants’ understanding of where their beliefs and practices regarding FGM come from to loosen the grip of such beliefs. Research happened through programs that were created by local community groups to address education and opportunities for community members, specifically girls at risk for FGM. Outcome expectancies play a substantial role in the maintenance of FGM practice and where rewards are seemingly low, sanctions might be perceived as high. This provided the program with crucial information on potential messaging to address sanctions while promoting rewards. Such discrepancies between the approval of a behavior and the practice of that behavior suggest that a norm influences the ongoing behavior. With research on FGM, these two tools provided researchers with data to support the triangulation of all data collected, specifically around indicators of injunctive and descriptive social norms.
In India, GARIMA targeted adolescent girls who are most impacted by the oppressive beliefs and practices related to menstruation. Their mothers were included in the primary audience along with their fathers, frontline health workers, and schoolteachers in the second tier. The social network map was used to help young girls express who influences them and their decision-making, attitudes, and practices. Development of these network maps aided researchers in defining relevant reference groups across social domains from family to friends and peers and the larger community to create programming that will target all domains in relevant ways and make real-time changes to ongoing programs where new messages and critical dialogue occur.
The visual participatory tools highlighted here were used in two ways for this study. First, during the behavior monitoring assessment conducted in the three districts in Uttar Pradesh, the tools highlighted three barriers to effective change around MHM: 1) feelings of “impurity” on behalf of the young girls; 2) absence of functional sanitation facilities or privacy for changing or washing; and 3) inadequate disposal facilities. Identification of these barriers established a relationship between menstruation and school absenteeism for young girls which equates to gender inequities and often leads to girls dropping out of school.
Second, an end-line evaluation was conducted to assess the relevance, effectiveness, efficiency, impact, and sustainability of the GARIMA program separate from the initial baseline assessment. Focus groups and interviews with key informants utilized these same participatory tools to reveal beliefs, attitudes, and restrictions coming from social norms perspectives and allow openness of communication across stakeholders, such as mothers, daughters, and peers. In comparison to non-intervention village adolescent girls, girls who have participated in GARIMA programs were better able to discuss a wider variety of aspects of menstruation and hygiene management, had more knowledge about puberty and reproductive body parts, and had more positive attitudes about gender (Ramaiya et al., 2019).
Using participatory methods, researchers work closely with program partners throughout the program cycle to meet the community in their program settings, reduce disruptions, and improve research compliance (Figure 8). Qualitative and participatory practices complement larger quantitative data gathering while providing the nuance of participant experience, measure impact in ways that may not be clear through quantitative data, and provide a means for evaluating necessary program changes. It is essential to the research design process that the type and level of participation are determined as to the best interests of the community and the research. See Figure 5 for an illustration of how participatory methods can be used during activities throughout each stage of research.

Qualitative methods are not inherently participatory and quantitative tools are not always non-participatory (Wallerstein, 2020). It is imperative that the research team consider how they engage the community as fully as possible when social norms are deeply embedded in a community, such as in the examples that we have provided, and where social change is dependent on shifting such deeply held beliefs. These tools may leverage research and program development to be integrated into larger community change. The activities can also catalyze change as part of participatory programs that can help community members to feel that they are part of the process of change. These visual tools are also a more inclusive means of promoting dialogue and discussion across knowledge and literacy levels, allowing for reciprocal interaction to better design, change, and adapt programs while also allowing room for innovation at the community level.
Participatory methods can be used to support equity in research designed to consider the agency and leadership of participant communities, culture-centeredness, de-colonial approaches, and other perspectives relevant to a particular community’s needs, concerns, and practices (Sprague et al., 2019; Wallerstein et al., 2017). In the examples we provided, communities are actively part of the research to develop formative program planning and implementation.
Conclusion
This paper set out to answer how visually informed participatory research tools (social network mapping and 2x2 tables) have been used to promote SBC and how these participatory mixed-method approaches can support the development of programs, monitoring and evaluation (M&E), and assess social and behavior change for public health issues around the world. These two tools support larger research and program agendas by assessing aspects of a social-ecological network and the influence of key social reference groups and individuals for social and behavioral communication.
Social network mapping and 2x2 tables support participants in developing an awareness of their social networks, the influences of key reference groups and individuals on one’s own understanding of a particular health issue, as well as larger social norms and communication networks that can perpetuate maladaptive and harmful health practices. Having a visual tool allows participants to manageably envision the complexities of who is in their social network and the importance that they place on their opinions or beliefs. Other standard qualitative and ranking methods, such as a verbal interview, may not have primed the participant to think so deeply and widely about specific individuals in their social networks. Similarly, asking about attitudes and perceptions within a standard focus group or interview may be less effective at parsing out the fullness of attitudes and behavior practices compared to using the 2x2 tables, where time is taken to fully appreciate each concept and the social consequences around breaking the norm. Each tool has been field tested in various global health contexts throughout the world and may be useful in a variety of research contexts where adding a qualitative, participatory component can enhance formative research and intervention programs as well as for M & E.
The use of participatory tools engages the intended audience in safely exploring sensitive, embedded notions that raise their awareness and create openings toward social behavior communication change. Community involvement may also serve to increase community accountability and support the tracking of change over time.
Limitations to any visual participatory methods such as we have discussed include their application to specific issues that may not be as relevant or engaging with all community members. Social network maps may conceptually differ in how researchers think to display them and how participants may conceptualize themselves within their social network. Designing the maps and pretesting them is essential to overcoming this limitation. 2x2 tables are limited in being a small-scale contingency table that accommodates such yes or no questions but is not flexible if perceptions are rooted in less distinct forms. Finally, participatory methods may be part of larger research endeavors in global public health but they cannot tell the whole story nor illustrate every aspect of such problems and efforts. Though there is data from many specific programs where these tools have been used, published research that shows their efficacy is limited. These tools are also limited to programs focusing on social networks and social behavioral communication around social norms impacting health practices and behavior. Many important health issues are less influenced by entrenched social norms that need to be addressed to see significant behavior change over time. Additionally, research to date has focused on health practices that have been of concern for decades. Not all relevant public health concerns are rooted in social norms, or are entrenched issues, and may not need such participatory interventions to consider how to untangle messages of influence.
Recommendations
Additional global health concerns that may introduce visual participatory research methods might include violence against children; issues around water, sanitation, and hygiene (WASH); positive parenting; gender socialization; or other health and human-rights issues, such as child marriage. General public health issues that may or may not reach a global scale can also benefit from tools that engage the audience as formative research and monitoring and evaluation support social behavior communication change. More localized issues in the United States, such as adolescent substance use (Salas-Wright et al., 2019), and risky sexual behavior (Schmiege et al., 2021) may be influenced by smaller-scale social networks. Community interventions to disrupt such behavior could benefit from a participatory approach to formative research and intervention design.
The research values and methods outlined in the paper provide strong encouragement to use visual participatory methods for data collection, analysis, and interpretation. To the latter points, member-checking results with a community stakeholder who can gauge the accuracy of findings can build trust and support validity. As for data collection, engaging participants in the development or conceptualizations of, and then pre-testing, visual tools will improve the accuracy of the data collection process. Researchers are encouraged to consider how participatory research tools could benefit their larger public health issue and approach. These tools may be an important part of initial program development when factors such as attitudes, health behavior, and social networks are implicated. They are also an accessible and flexible method to support ongoing monitoring and evaluation for adaptive changes during programming. Participant data can be triangulated with other data and add relevance as well as perspective to large-scale public health issues as policy and practice are implemented.