Introduction
Endometrial cancer is a cancer of the inner lining of the uterus and the most common and most lethal gynecologic cancer in the U.S. (Morice et al., 2016). It is one of the few cancers increasing in incidence each year. Black individuals have a 2-fold higher mortality than White people, in part due to delayed diagnoses (Hicks et al., 2024). Recent evidence recommends updating clinical guidelines to favor biopsy over ultrasound as a more effective method for early detection of endometrial cancer among at-risk Black individuals exhibiting the key symptom of endometrial cancer—postmenopausal or abnormal bleeding (Clarke et al., 2018; Doll et al., 2021, 2024; Gross et al., 2025; Orellana, Pike, et al., 2025). To help address this disparity and raise awareness about endo
metrial cancer symptoms and diagnosis, we developed a culturally relevant educational toolkit for digital dissemination. In response to the severe lack of gender diversity in endometrial cancer health information, we targeted gender-expansive individuals (defined as transgender, nonbinary, gender non-conforming, and all other people who do not identify with cis-normative gender roles) as consultants and research participants in toolkit creation.
Community Consultants
To develop the toolkit, we collaborated with four community consultants: two Black cisgender women endometrial cancer survivors and two Black gender-expansive health advocates. The survivors included one woman with a pre-menopausal endometrial cancer diagnosis and one woman with a post-menopausal endometrial cancer diagnosis, both of whom had experience in community health promotion and endometrial cancer advocacy. The gender-expansive community consultants were both non-binary – one a board-certified OBGYN with a gender-diverse clinical practice and one an artist engaged in uterine health promotion. Our endometrial cancer survivor consultants have been involved with our team on various projects over the years; one was initially recruited as a research partner after being a patient of the team’s Principal Investigator, and the other was referred by a research colleague. We reached out to assess their interest in consulting on this project, which would include providing feedback on study and toolkit materials and attending meetings. Our gender-expansive consultants were identified through professional networks and approached through “cold” outreach. All consultants agreed to an hourly rate, and signed contracts as university vendors in order to be paid hourly by check.
To avoid common challenges in community-engaged dissemination work, we designed our communication processes with guiding values of transparency and consistency in demonstrating the value of consultant input. For instance, consultants were involved throughout the entire research process. At the start of the project, we held virtual meetings monthly with each of our consultant teams to discuss recruitment strategies and materials. Each meeting focused, alternately, on either cisgender or gender-expansive populations to ensure our strategies and materials addressed both populations of interest. We were guided by consultants that our materials needed to be created directly for the gender-expansive community rather than repurposing cisgender materials by simply changing gendered language.
Quarterly meetings were held with our community consultants and the entire research team to discuss the overall research approach and provide project updates. To maintain equity, we addressed all members by their first names, and we acknowledged that everyone brings a different expertise to our project. Meetings were facilitated by the authors, MAO and KMD. At each meeting, consensus on next steps was reached by the end of the meeting, after MAO or KMD proposed solutions based on attendees’ input and there was agreement on the proposal’s feasibility and alignment with our research goals. A summary of each meeting was emailed to all stakeholders.
After the meetings to develop materials were completed, materials underwent an iterative review process via email prior to final dissemination. Community consultants also used their personal and professional networks to disseminate materials and identify other organizations to distribute our educational materials. Finally, consultants provided feedback on our scientific dissemination products. They reviewed and were included as authors in abstracts, presentations, and manuscripts.
We did encounter administrative challenges in executing this community-engaged research. For instance, at one point, payments to consultants were delayed as the PI’s large university system was transitioning to a new payment system. We rescheduled meetings or did not ask consultants to attend meetings if their payments had not been processed on time. In addition, a contract review and negotiation process was necessary to clearly outline roles for the consultants that aligned with their desires.
Creating the Educational Toolkit
A mixed-methods study was conducted to inform the toolkit’s content. The quantitative component involved analyzing medical records from Black patients across a 10-hospital health system (N=3455) to identify risk factors affecting the quality of transvaginal ultrasound measurements used to assess endometrial cancer risk and need for biopsy (Orellana, Pike, et al., 2025). The qualitative component involved four focus groups (N=19) with three different demographics of Black people at risk for endometrial cancer: 1) Black cisgender women aged 35-49 with a history of abnormal uterine bleeding (N=6), Black women aged 50+ (N=8), and 30, and two sequential focus groups with the same gender-expansive individuals aged 35+ (N=5). In the qualitative component, we identified barriers and facilitators to endometrial biopsy (a key component of endometrial cancer diagnostic work-ups) (Alson et al., 2025; Orellana, Williams, et al., 2025) and gathered input on the content (the type of information) and the structure (how information is presented and communicated) of the proposed toolkit. Details about the focus groups and their results are provided in prior publications (Alson et al., 2025; Orellana, Williams, et al., 2025).
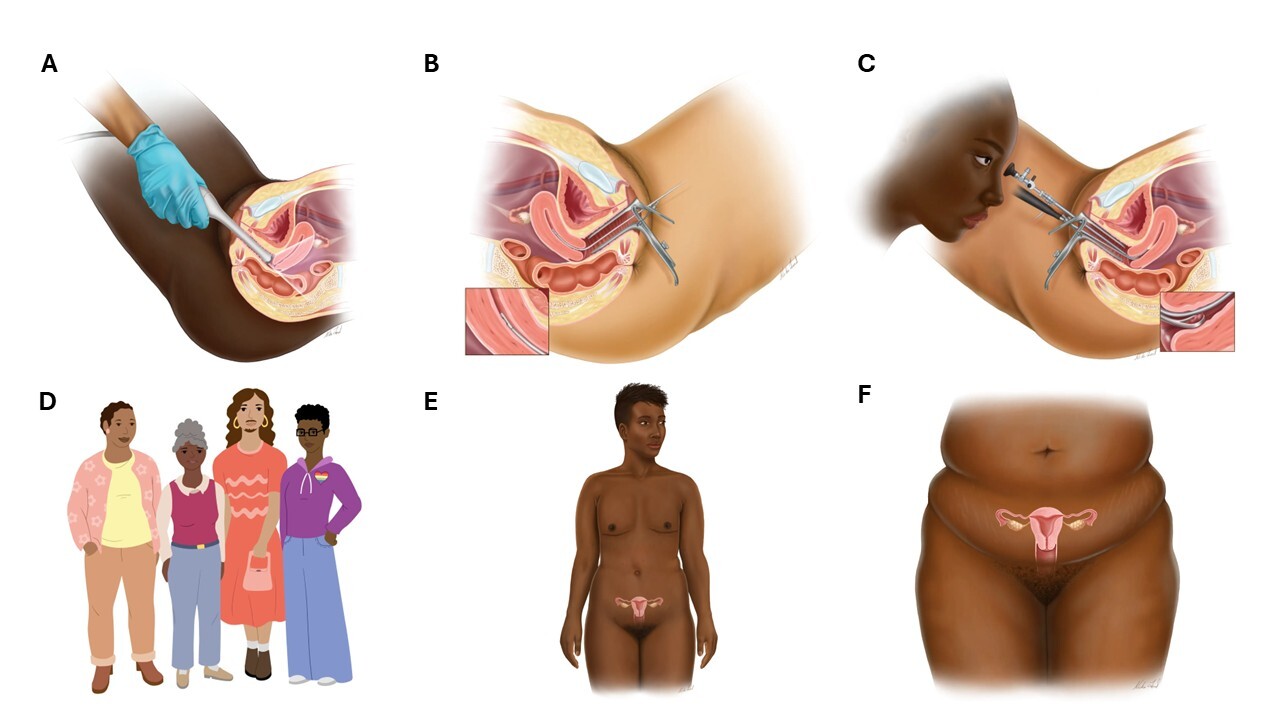
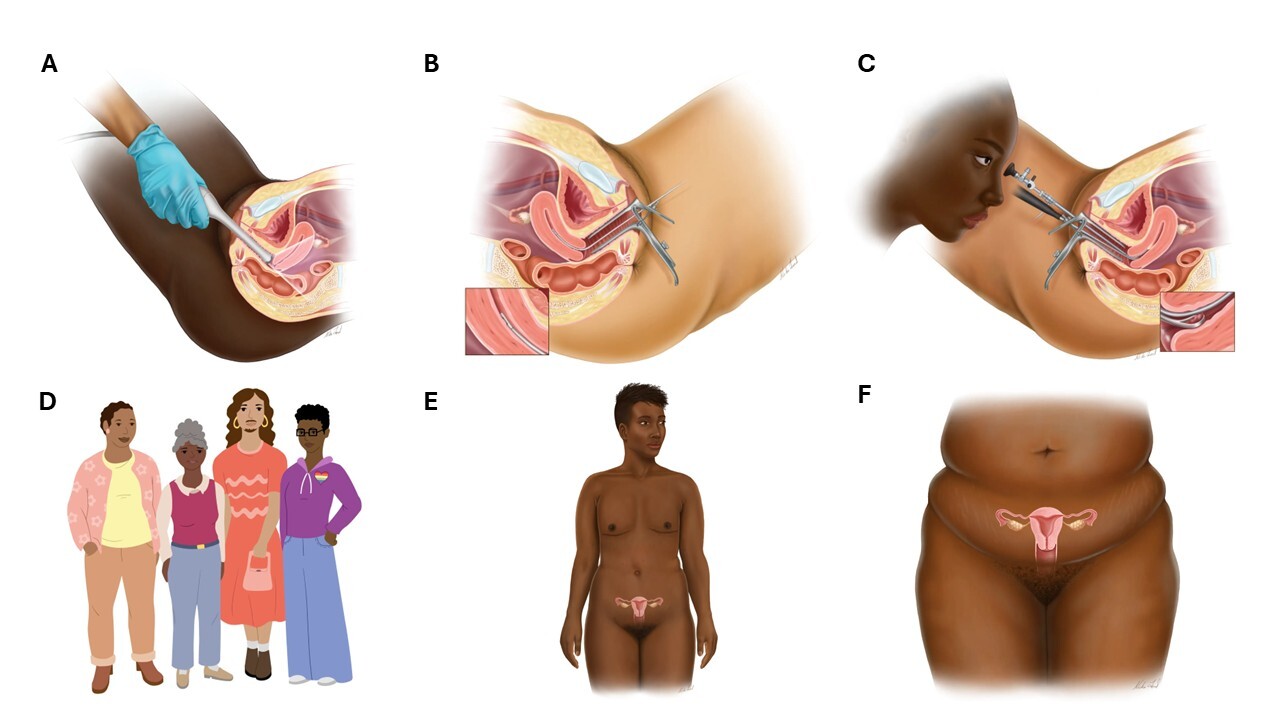
One key focus group theme was the need for images of Black people of all ages, sizes, and skin tones when depicting gynecologic anatomy and procedures. We hired a medical illustrator to create six new illustrations of Black people undergoing gynecologic procedures, Black people with a uterus, and gender-expansive graphics. Images are shown in Figure 1. Another key theme was to shift our language when discussing suggestions for early biopsy to set a more patient-centered, empowering tone for the toolkit. To do so, we changed our original language of ‘biopsy-first’ to ‘risk-based.’ The final theme about content was the need to supplement endometrial cancer information with practical advice for individuals seeking gynecologic advice to reduce barriers to care. We created content including preparation checklists, post-procedure recovery advice, and more. Regarding structure, recommendations included using infographics, video content, and a comprehensive ‘one-stop’ webpage.
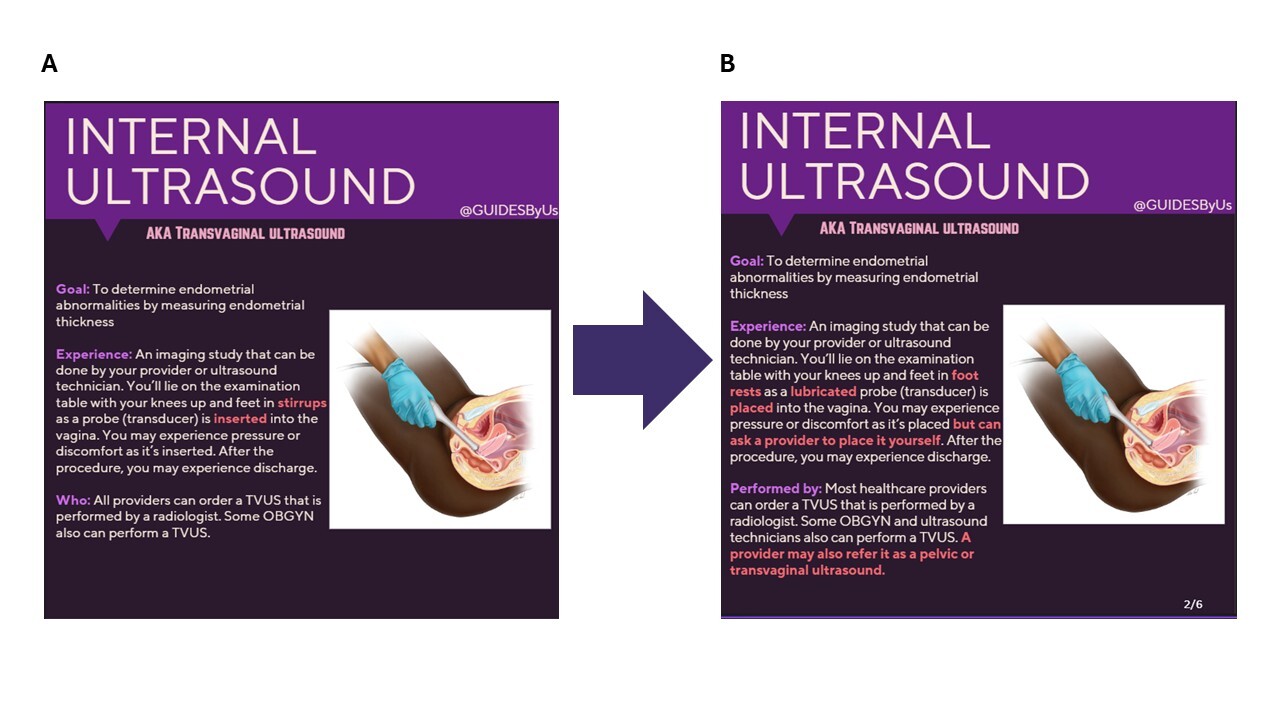
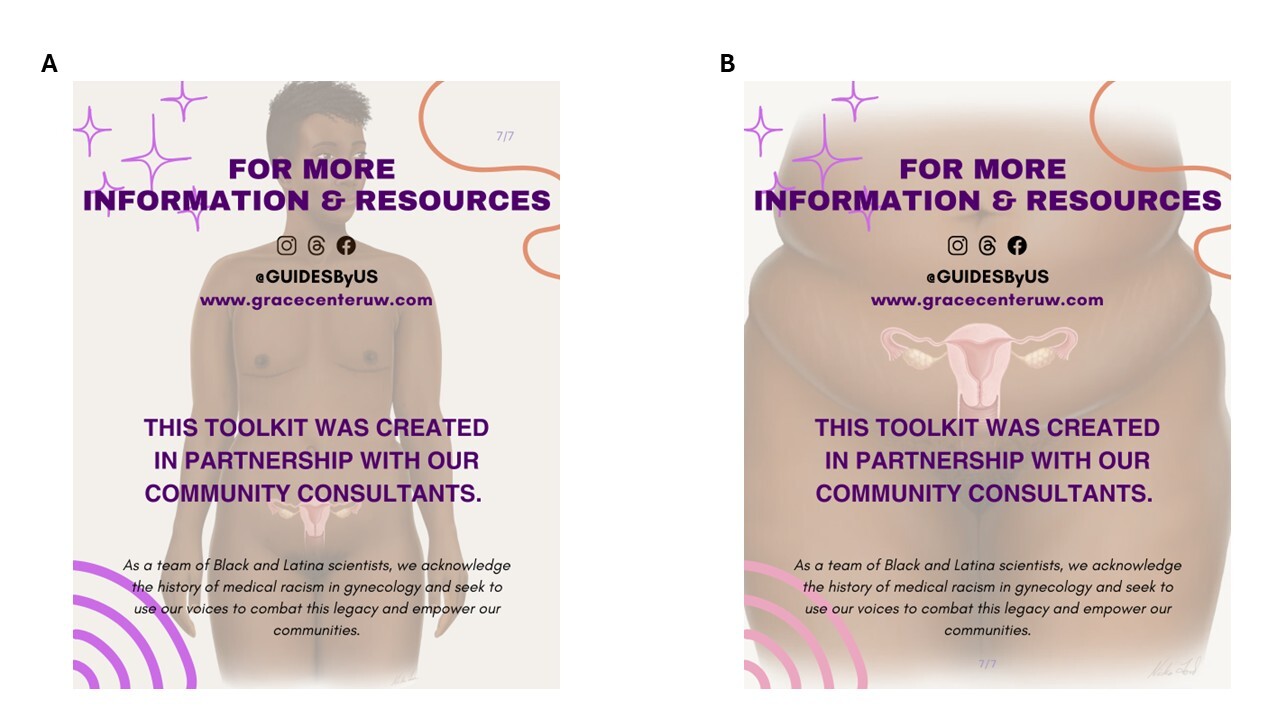
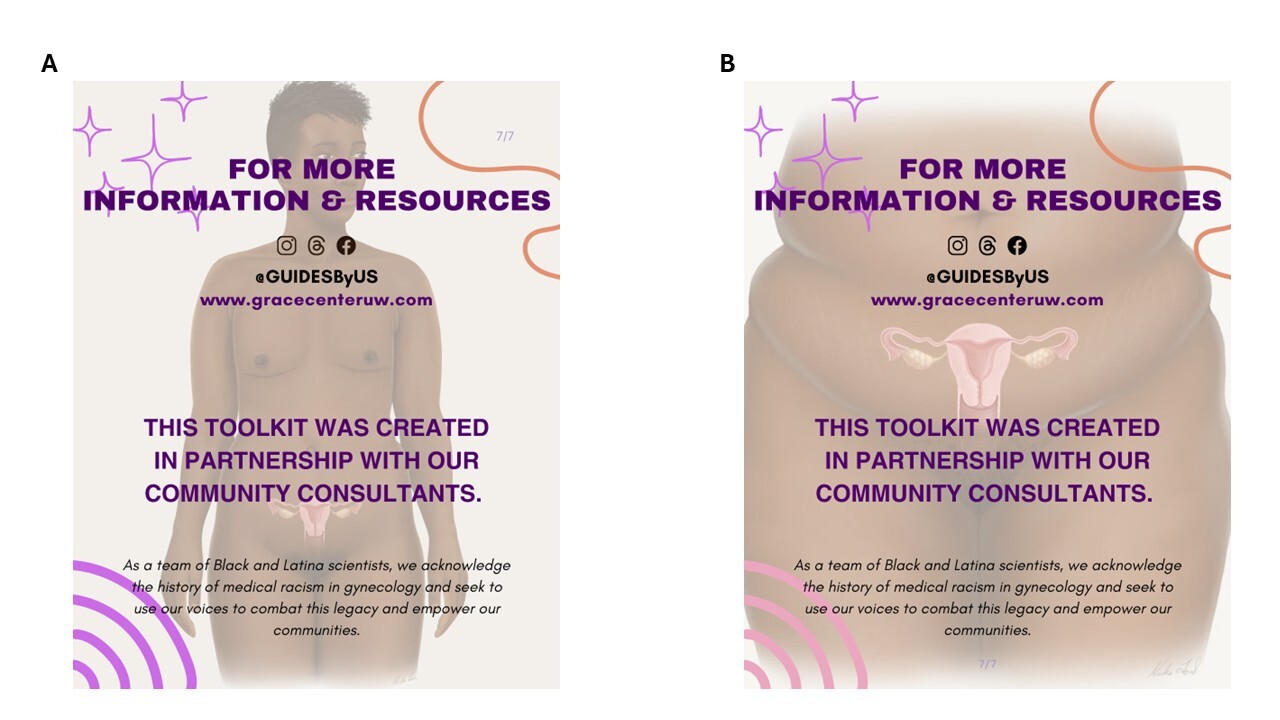
The infographic components underwent an iterative creation process with team members and community consultants. First, text-based information was developed based on current literature and the mixed-methods study for use in educational materials addressing endometrial cancer background, risk factors, and related diagnostic procedures, including diagnostic accuracy. Text was also developed to teach about gynecologic procedures and provide guidance on interacting with gynecologic providers. Second, infographics that incorporated the text and medical illustrations were created in Canva. At each step, elements were presented to community consultants and refined with their feedback. Figure 2 shows examples of changes made based on community consultant input, resulting in more inclusive language, greater agency, and improved readability. For two infographics, custom versions were created for cisgender women and gender-expansive audiences to reflect the disparate consultant preferences. Figure 3 shows one set of custom versions.

Regarding video, we recorded two elements: 1) author KMD delivering a 15-minute presentation on endometrial cancer, focused on risks to the Black community; and 2) a Black endometrial cancer survivor (one of our consultants) sharing her diagnostic journey. We created several 90-second clips for social media from both videos and retained full versions for posting on YouTube. We have included an edited video of our community consultant, an endometrial cancer survivor in Supplementary Materials. For the webpage, we created a new webpage on the research center’s website to house all toolkit components and links to original content. We conducted three implementation waves – pilot testing, decision-making facilitation, and a final community partnership phase – described below.
Toolkit Dissemination
Wave 1 – Pilot Testing of Knowledge Translation Components
Wave 1 of dissemination focused on sharing the knowledge translation elements, including toolkit infographics, conversational text, and video clips. We aimed to identify how content performed on different social media platforms. We collaborated with the Endometrial Cancer Action Network for African-Americans (ECANA), to support dissemination. ECANA is one of our longstanding community partner organizations that was founded by author KMD. We have maintained a collaborative relationship with ECANA. From September 2024 (Gynecologic Cancer Awareness Month) through February 2025, a total of 13 posts were shared on Instagram, Facebook, and Threads via our social media profile (@GUIDESByUS). These platforms were selected due to the team’s familiarity with platforms and the ability to cross-post on other platforms, which maximized our reach and maintained content consistency.
Our posts included a mixture of reels (videos) and posts (carousels of images/infographics). For each post, we tracked metrics including views, likes, shares, saves, and interactions (the total of likes, shares, and saves). For one of our lower-performing posts, GRACE Center Research, we tested using a paid ad to gain more followers of our account. We were able to pay for the post through a feature called “boost post”, which enabled us to target a selected demographic: U.S. females ages 35-65. We set our goal for the “boost” as “visit our profile” and set a budget of $65 over a period of 5 days. Both budget and timeline could be shifted to increase or decrease the estimated impressions. Lastly, we were able to choose the platform on which we wanted our ad posted. Boosting did increase our interaction and followers in our pilot period.
At the end of this pilot testing period, we found that interaction patterns varied by post content. For example, the post with the most shares was “Let’s learn about endometrial cancer”, while “How to prepare for a gynecologic visit” had the most likes and saves. Use of the paid ad modestly increased follower count (n=29) and more strongly increased views (64% increase), making it our best-performing post (highest interaction). Instagram was found to be the most successful social media platform.
Wave 2 – Decision-Making Facilitation
Wave 2 involved connecting a decision-making aid to each of our knowledge translation elements. An interactive quiz format was chosen, given the focus group findings of a desire for personalized risk information and a sense of agency. We developed six questions and enabled branching logic based on responses. Questions asked about endometrial cancer symptoms, menopausal status, and age. Quiz results were categorized into three groups: minimal risk, questionable risk, and high risk for endometrial cancer (See Tables A1 and A2 for quiz questions and outcome scripts). Each outcome was outlined and tested on the platform to yield the appropriate final results. A shortened (Bitly) link and QR code were created for the quiz and incorporated into a final infographic slide to be embedded with the knowledge translation material. The link was also added to each social media profile and the webpage.
Wave 3 - Engagement and Dissemination via Community Organizations
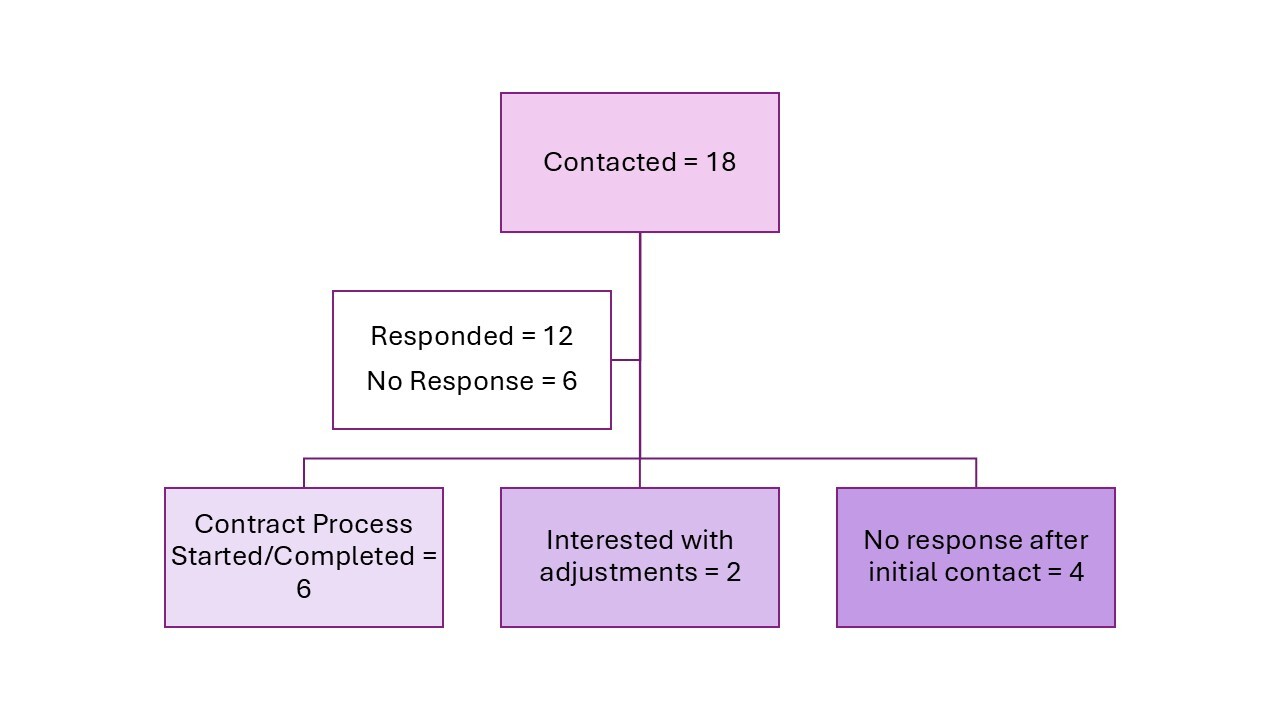
In the final wave, we sought out community organizations and advocates focused on Black health with various areas of focus, including uterine fibroids, gynecologic cancer, Black women’s health, Black gynecologic health, reproductive justice, and LGTBQ+/gender-expansive health and well-being. Potential partners were selected based on an active Instagram presence and a history of sharing health information. Author MAO contacted each organization based on instructions in their online profiles, including contact via email, Instagram message, or contact form. Contacts included a message with a brief overview of the research center and the study, along with an invitation to meet and learn more. They were contacted up to three times before discontinuing outreach. For those engaging, our proposed partnership contract included sharing the educational toolkit on their platform of choice, with $100 per post for up to ten posts, and an agreement to share one month of tracking metrics with our team.
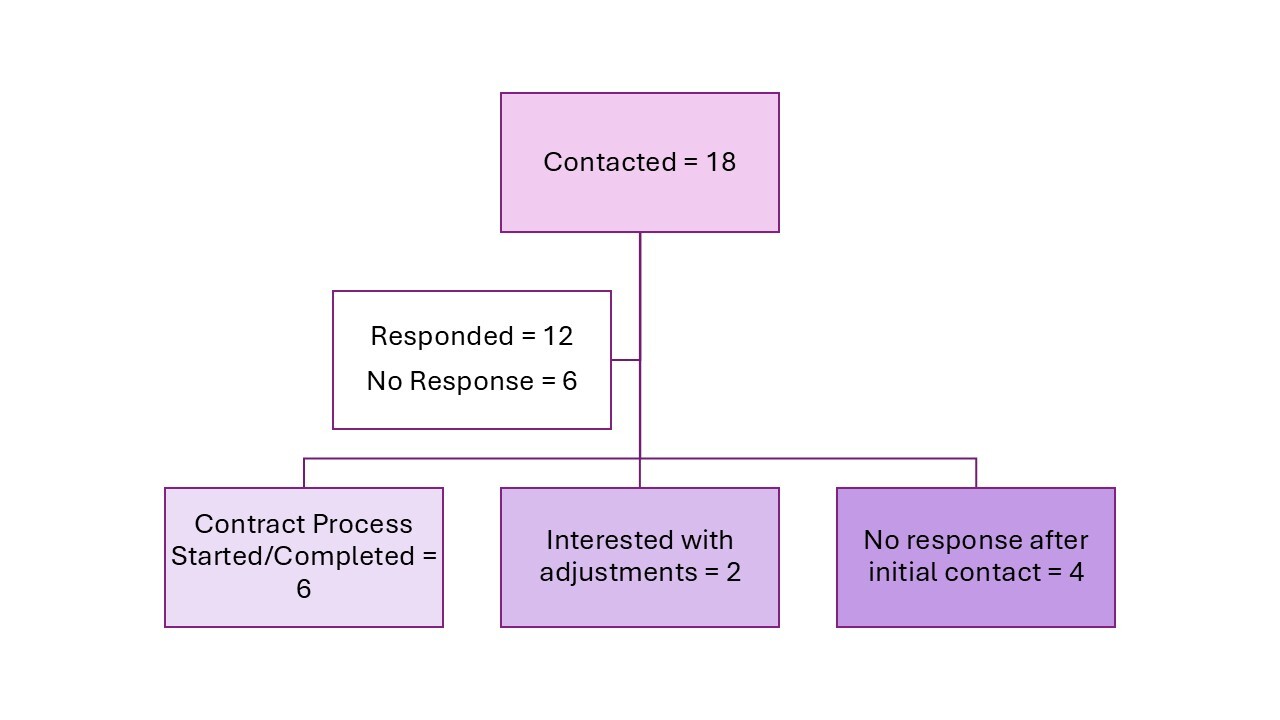
Eighteen community organizations and advocates were contacted, with six ultimately partnering with us. The contacting process and outcomes are outlined in Figure 4. Our partners include an endometrial cancer survivor-led non-profit (ECANA), a uterine fibroid patient advocacy group (The White Dress Project), a Black female health platform (Black Girl Health Bank), a Black gynecology platform (The Black OBGYN Project), and two health advocates focused on gender-expansive identities (Kuluntu Reproductive Justice Center & an independent gender-expansive advocate). Our partners were allowed to choose the content and the final acknowledgment slide they wanted to use, from among all that we created. Posts could be reformatted to reflect the organization’s visual style, but the content remained the same. Three partners requested modifications to the format and colors, and one asked for image descriptions. An LGBTQ+ cancer organization expressed interest in our content but was unable to participate due to time constraints. However, they offered content suggestions to add to our gender-expansive material, which we developed and shared with our gender-expansive community consultants for iterative feedback before sharing the updated content with the partnering organizations. Selected posted material by community organizations and advocates is summarized in Table 1.
Wave 3 ran from May 14 to September 30, 2025, concluding with Gynecologic Cancer Awareness Month. The final date for collecting metrics was October 30, 2025. All organizations posted on Instagram. For all organizations, we gathered views, likes, shares, saves, and interactions. Our top-performing post (@GUIDESByUS) was “How to Prepare for a Gynecologic Visit,” and had the most saves, mirroring our Wave 1 metrics. Overall, top-performing posts differed across all organizations (Table 2). For ECANA, the GRACE Center Research post was the top performer, aligning with this group’s familiarity with endometrial cancer and their interest in current research. For the gender-expansive partners, “How to Prepare for a Gynecologic Visit” and “Testosterone + Uterus: what do we know?” were the most popular. For the non-cancer-specific health organizations, “How to Prepare for a Gynecologic Visit”, "Endometrial Cancer Survival/Disparities, and “What is Endometrial Cancer?” were the most popular. Similar to Wave 1 results, posts about general gynecologic visits or procedures were more likely to be saved than posts about endometrial cancer-specific information across all groups. We are unable to determine if adding the decision aid link and QR code influenced our performance, as we have no comparison wave with the metrics available.
For the quiz, we received a total of 34 responses (Table 3). We could not determine which responses came from which organization due to software limitations. Among our respondents, 79.4% were under 55 years of age, 38.2% were experiencing menopausal symptoms, and 64.6% experiencing severe symptoms. When analyzing response categories, 14.7% were minimal risk, 47.1% were questionable risk, and 5.9% were high risk.
Study Implications
Using a mixed-methods, community-engaged approach, we developed and disseminated a culturally relevant endometrial cancer educational toolkit for Black women and gender-expansive people. The design was guided by feedback from the focus groups, with all posts using a consistent visual style and wording. Through our community-engaged process, we moved from an endometrial cancer-focused plan to a broader, more holistic approach that addressed common barriers to gynecologic care. These additions proved popular across multiple platforms, underscoring the value of community engagement in health promotion. The use of our focus groups in identifying our toolkit content was successful. The content resonated with each or our different organizations. For instance, organizations focused on Black gynecologic/women’s health had high interactions on posts focused on preparing on gynecologic visit and endometrial cancer information. Our gender-expansive partners’ audiences were interested in the effects of testosterone on the uterus. This post was created from a direct discussion with a community partner. Through this successful, collaborative process, we have built trust with our community partners and a path towards long-term partnership with our research center.
We have created this educational toolkit as a living document to continue empowering communities at the highest risk for endometrial cancer by sharing information. With regard to our decision-making quiz, though our overall number of respondents was modest, most were under 55 and premenopausal, a key demographic to reach in order to share information prior to the age at which endometrial cancer risk is highest. By centering community voices, we have addressed gaps in endometrial cancer awareness and created a resource that can continue to grow and be shared across communities.