



Background
Traditional research dissemination in public health emphasizes strategic communication to academics, policymakers, and public health practitioners, with other groups as secondary audiences (Sofaer et al., 2013). In contrast, participatory dissemination centers those who participated in the research and those most affected by the issue of concern as both key audiences and valued collaborators in dissemination, while also keenly attending to interest holders who are most directly positioned to change policies and systems around public health issues (Cunningham-Erves et al., 2020, 2024; Gollust et al., 2025). There has been relatively limited uptake of proactive planning of dissemination in public health (Brownson et al., 2013; Kwan et al., 2022), despite awareness of the importance and benefits of community collaboration for research dissemination (Mosavel et al., 2019; Wallerstein et al., 2017), the emerging literature on best practices (Cunningham-Erves et al., 2020, 2024; Gollust et al., 2025), and the range of roles that community participants might play in dissemination (Chen et al., 2010). From the literature and our own experience, we see that relationship-building is the common thread at the heart of all participatory work, including effective participatory dissemination efforts (Cunningham-Erves et al., 2020, 2024; Wallerstein et al., 2017). However, we are struck by how little this literature explicitly addresses how it might feel to engage with distressing public health data as it is disseminated. Given that public health issues are typically the result of and/or exacerbated by long-standing structures and systems (e.g., racism, gender inequities) that create harm, in this paper, we explore what is needed to make a healing space that allows us to engage with those harms.
At the outset of this project, our intention was to conduct a community planning process to bring a COVID-19 memorial artwork to an institution and a neighborhood, culminating in a launch event. It is important to note that our project was not in response to a research question or born from an existing academic-community research partnership, but it does shed light on processes that are relevant for such projects and partnerships. Through the work we will describe, we learned about the deep meaning and utility of creating shared spaces for grief and celebration. We argue that these spaces—built for and by community members affected by public health issues through participatory mechanisms—are a critical element that has yet to be recognized in community-facing research dissemination efforts. Integrated into participatory research dissemination, these spaces have the power to replenish and strengthen people made vulnerable to and by public health issues, and to grow the networks needed for ongoing resilience and participatory action in public health.
The Need for Healing Spaces
Despite the profound loss of life during the first year of the global COVID-19 pandemic, most people’s ability to mourn or process grief was severely limited. The mourning practices of nearly all religions and cultures include a forum of communal gathering. For most of 2020, public spaces were closed and mass gatherings prohibited by most jurisdictions. At the individual level, loved ones’ grief was exacerbated by further loss of tradition, ritual, and company (Norton & Gino, 2014). In the professional realm, those tasked with responding to the pandemic had little time to contemplate the enormity of the loss unfolding, individual connections to those lost, or the sense of “failure” implicit in each death.
Later, as the focus of efforts moved from response to recovery, public health practitioners, frontline and essential workers, first responders, and families pivoted from one crisis to the next, overlooking widespread emotional depletion. As one example, a 2024 national survey of state and local public health workers found that 70% reported at least one symptom of burnout, and 20% reported near-constant symptoms of burnout (de Beaumont Foundation, 2024). For many in these communities, the systemic pressure to keep moving forward precluded the necessary processes of grieving and restoration.
While the COVID-19 pandemic has been unusually devastating–affecting the health and lives of so many people globally–traumas, erasures, and systemic harm are woven throughout many, if not all, public health issues. For this reason, we believe that attending to steps that can be taken toward community healing is a worthy consideration in all community-partnered public health projects, not only when it comes to historic moments in public health, like the COVID-19 pandemic.
Contributions of Art and Memory
From the beginning, our project was focused around an artwork, Trace: A Memorial. Research indicates that art can play an important role in recovery from collective trauma specifically (Saul, 2022), and also in community development more generally (Sonke et al., 2019). The experience of an artwork can mobilize kinesthetic, sensory, perceptual, and symbolic modes of communication, allowing us to engage in ways that language alone might not (American Art Therapy Association, 2026). Research highlights several benefits of integrating the arts into community development efforts, including getting people involved who otherwise might not participate, raising awareness of issues in new ways/(re)building connections to issues, promoting community building by facilitating dialogue (Catalani et al., 2022; Sonke et al., 2019), as well as reducing stigma, addressing trauma, and nurturing cultural identity and social connection (Hand & Golden, 2018; Sonke et al., 2019). These efforts can also enhance trust building, which can be achieved through a range of approaches such as creating safe spaces, listening, transparency, embracing differences, and practicing authenticity (Greene et al., 2025; Hallmark et al., 2022; Lansing et al., 2023; Sanchez-Youngman et al., 2023).
Memory and memorializing are also at the heart of this artwork, and as we will describe, our conversations with community members underscored for us the importance of the fact that this was not just any artwork, but an artwork that engaged us all in remembering. Memory scholars describe how memorials can work to both hold space for the ongoing suffering created by events of the past (without striving for closure) and offer opportunities to create and expand “communities of memory” through public memory work (Atkinson-Phillips, 2018, 2022). Communities of memory are formed around memorials by people who share the experience of a past event or period, but who need not have the same memories or experiences of it (Atkinson-Phillips, 2018). Public memory work, on the other hand, encompasses efforts to shape how history is remembered for better and for worse or to correct wrongs, like the movement to remove a statue of J. Marion Sims, a once celebrated gynecologist who experimented on enslaved women, from New York City’s Central Park (Domonoske, 2018). These activities overlap with, but also diverge from, the action-oriented work of participatory research, which is typically focused on problem description, intervention design, solution creation, and policy advocacy.
Setting
Our context for this work is New York City, and specifically Central Harlem near the corner of 125th Street and Lenox Avenue. In that location is a 14-story brick office building, originally built in 1874 and renovated to its current incarnation in 1998. Since 2016, several floors of this building have been home to the CUNY Graduate School of Public Health & Health Policy (CUNY SPH). On the ground floor, in a storefront space, resides the Harlem Health Initiative at CUNY SPH (HHI). The Harlem Health Initiative’s primary goal is “to improve the health and well-being of the Harlem community by supporting its existing community-based organizations.” Trace lives just inside the storefront windows of HHI’s community-oriented open space.
In this paper, we will tell the story of bringing Trace: A Memorial to this place, the processes that brought forward the creation of a space for collective remembrance, recognition, and grieving (CRRG), and how dedicated participatory work both builds and sustains the CRRG space. We will then describe what we see as key practices of this kind of space-making, strengths and limitations of this approach, and how the thoughtful creation of CRRG spaces might benefit participatory research dissemination efforts. First, though, we describe what Trace: A Memorial is.
Introduction to the Artwork by Nyssa Chow
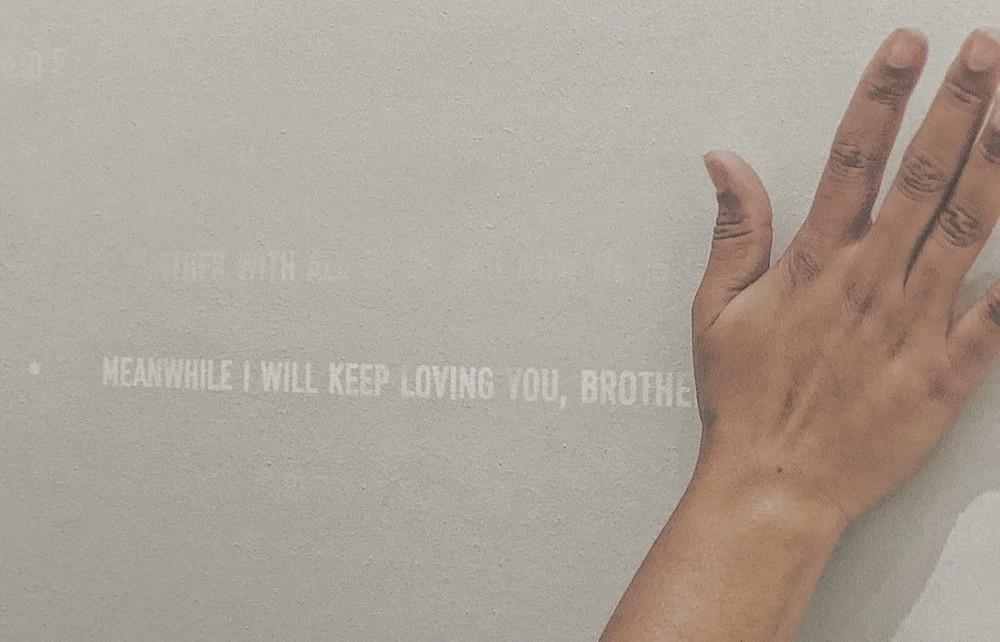
Trace: A Memorial was first created in 2021 as a response to the first year of the pandemic and lockdowns. It is a memorial to one hundred Black and Brown essential workers lost in the early months of 2020 to COVID-19 (The Essential Workers of the Coronavirus Pandemic, n.d.). All would have died without being touched. What you encounter first is their absence—a large blank wall that blends into the environment. Written on the wall in heat-sensitive paint are single-line/phrases of memory that their loved ones shared about them after they had been lost, along with their names. The writing is invisible at room temperature. In order to bring them into visibility, you have to lay hands on the wall, letting the body heat of your touch solicit permission to see their names. Once the names cool, they fade to invisibility again.

Touch was the thing most denied to everyone, including the dying, during the pandemic. It feels particularly moving that the intimacy and warmth of touch are the very things that will reveal them now; that visitors must implicate their bodies and solicit permission to commune with them here.
For the people who loved them, memories remain; grief transforms daily life into a palimpsest of what was, and what might have been. This work transcribes that trace. To recreate the experience of that trace, these phrases of memory will appear throughout this article. To distinguish them from the main text, lines from loved ones will look like this:

Trace: A Memorial is an invitation to visitors to meditate on the connection between their own bodies and those workers upon whom all our lives depend—our shared precariousness in the face of disease, yet our differential vulnerability rooted in the reality of precarity. They had no choice but to keep working while others could shelter in place. As each phrase of memory is revealed, we are asked to reckon with the present continuous reality of systemic vulnerability—a confrontation with the ways that, in our current system, our own lives depend on the ongoing precarity of others. The tragedy is not just that they died, but that while we were all vulnerable to COVID-19, they were differently vulnerable to this kind of loss to begin with. It is an invitation to form a moment of relationship; to experience these lost lives as grievable; to rescue both their loss and the conditions of their loss from abstraction.
This memorial is also conscious of its time, post-George Floyd protests, when so many hurt and dying Black and Brown bodies were relentlessly and repetitively on display. This monument seeks to deny the viewer the Black and Brown body itself. There are no images in this memorial. There is nothing to photograph. Anything the visitor takes from this experience, they will carry in their body.
One perspective on a memorial is that it commemorates a single, bounded event in the past—a historical event that begins and ends, and the associated grief. For Trace: A Memorial, my intention was to rethink what is possible to remember and reimagine the boundaries of what we call an “event.” Instead of death as a singular event, the intention was to posit the deaths of these Black and Brown “essential workers” as part of a present-continuous—a history of structures, systems, and processes that implicates us all. In other words, an act of communal/participatory remembering can pose different questions: What are the conditions that made this death possible? What is my relationship to this? Who or what do you feel a duty to remember? This is a participatory artwork as it requires the visitor’s presence to exist; the artwork is the encounter itself, not the object on the wall. The grief we are truly called to feel is not for the death alone, but for the ongoing differential vulnerability that made this loss possible.
Trace: A Memorial is grounded in the assertion that a memorial about Black and Brown essential workers and COVID-19 must be honest about, attend to, honor, and represent what their loved ones are grieving. The loss of loved ones, but also the unnamed losses, the illegible griefs, the invisible harms that attend precarious lives. What must be memorialized is what they hope will be remembered, what they hoped would have been known, what they wished had mattered but did not, and may not still. The content of this participatory remembering/memorializing must be situated within the present continuous of systemic vulnerability and the historical longue durée that carries these moments into our present. The intention is that these rememberings not be disembodied from their embodied and situated knowledges; that their losses be framed, not as a singular event, but rather seen, known, and recognized to be part of a process, one that began long before COVID-19 and will continue without accountable intervention at a structural level. I hope to offer Trace: A Memorial (hereafter Trace), not as a monument to the past, but of a living present, for it is not past—its continuity remains unbroken.
Methods of Reflection and Analysis
To generate the insights of this paper, we did not use formal research methods. Instead, we 1) built relationships with one another through meetings and the collaborative work described in the following sections (and in part through our own informal processes of shared remembering), 2) used periodic collective reflection and discussion (including in the process of recording interviews for the brief film about this process which is under development), and 3) collaborative writing to surface the “findings” presented in this article. Note that, unless otherwise noted, the quotes used throughout the article come from these discussions and reflections. Additionally, though they are not as central to our analysis as our own experiences, we do also reference learnings from the brief survey (n = 18) and semi-structured interviews (n = 8) about event attendees’ experiences with Trace that we used to refine the Resource Guide and Engagement Toolkit. Emma Tsui and Arielsela Holdbrook-Smith analyzed these interviews in collaboration with two MPH students using a modified Framework Method approach (Gale et al., 2013).
Consistent with qualitative, participatory, and community-engaged research traditions, we approached Trace as a reflexive, co-produced process shaped by positionality, institutional power, and structural constraint (Finlay, 2002; Wallerstein et al., 2023). Rather than treating reflexivity as a post hoc disclosure, we embedded structured reflection into decision-making processes across project development, installation, and dissemination. This approach aligns with calls for explicit examination of power in community-academic partnerships and equity-centered research. We briefly describe our positioning in footnotes when our roles first come up in the stories we narrate below.
Findings
An Iterative Process of Space-Making
In the story that follows of how we created a CRRG space around Trace, we hope that readers will attend to three core practices that are interwoven throughout: 1) Practices of shared remembering that allow the emergence of personal experience alongside professional experience and that help to knit new kinds of relationships, 2) Practices of orienting toward potential participants’ diverse interests in this kind of space-making to create a wide tent, and 3) Use of the Council of Elders Framework to give local interest holders permission to help author the space, to ensure the integration of cultural knowledge from those made most vulnerable by the public health issue, and to center the people who “do the work” (to address this public health issue) locally.
Inception
Memory as Focus. The story of Trace’s arrival at CUNY SPH began with a single conversation. After reading about Trace and learning from Nyssa Chow[1] that it had no public home, Emma Tsui[2], a faculty member at CUNY SPH, approached Deborah Levine[3], the Harlem Health Initiative’s Director, in hopes of partnering to create a home for Trace. The response of the HHI team[4] was immediate and deeply personal. HHI recognized Trace as an expression of its mission to anchor equity and community partnership at the school. The team also dreamed of ways to not only install the artwork but to support ongoing engagement with it. This small group began meeting on Zoom and in person periodically and found that talking about Trace led almost inevitably to sharing how the early years of the COVID-19 pandemic had shaped us and how we lived with those memories now. The portion of our initial meeting devoted to this spontaneous experience of shared remembering operated in a different, quieter, and more attentive register than that of typical professional meetings, and began to knit trust and care into our group dynamics. Through these meetings, HHI, Emma Tsui, and Nyssa Chow resolved to have Trace installed permanently in the HHI storefront space.

Building Partnerships. Actualizing Trace required numerous internal and external partnerships–some of which were facilitated by a similar kind of shared remembering and others not. These are significant not only for their pragmatic importance but also because they helped shape the artwork’s experience. The small team, described above, cultivated institutional buy-in and laid the groundwork for engaging external partners. These early conversations involved CUNY SPH senior leadership, including the director of facilities, the CUNY SPH Foundation, the NYC Preparedness and Recovery Institute (PRI), of which CUNY SPH is a key partner, and Danielle Greene[5], PRI’s Senior Advisor. Throughout this period, Nyssa Chow worked closely with the team and school leadership, providing real-time input on layout, accessibility, engagement, intent of the artwork, and messaging.
Within this group, we found that the concept of Trace tapped into a shared sense of curiosity and humanity, but that these conversations were confined to a more professional register. Given this, strategically, we saw the importance of approaching each conversation considering what mattered most to the interest holders involved. For senior leadership, communications emphasized how Trace reinforced the school’s commitment to social justice and mission to advance health equity through collaboration. For facilities staff, discussions prioritized the logistics of safely hosting a tactile and participatory installation. Focusing on Trace’s potential as both a public health teaching tool and a community-centered memorial, the Foundation helped to secure resources and amplify the work. PRI, particularly Danielle Greene, recognized Trace’s value in pandemic memory and resilience-building and became a partner, committing both staff time and financial resources.

Power Sharing. At this point, the artwork had champions and a path toward installation. However, to create the space we were envisioning, we needed communities and constituencies that might participate in shaping and joining this space. The Harlem Health Initiative led this process by mapping its partners based on relationships developed over the past five years, with particular attention to partnerships formed during COVID-19 and its aftermath. This list was reviewed through a Council of Elders lens (see Box 1) and shared with the artist and internal school staff, who were asked to identify gaps and suggest additional voices. The guiding question throughout this process was, “Who is missing?”
This list was also shared with the CUNY SPH Dean’s Advisory Council. This council includes organizations and individuals aligned with the school’s mission and serves as a key bridge between the school and the broader New York City community. Members provided feedback, offered connections, and helped strengthen alignment between Trace’s goals and the school’s academic and service commitments. Following this review, Trace was presented to the health committees of three local community boards. These committees provided input on design, language, accessibility, and community relevance. Once feedback from these committees was incorporated, the project was brought to the full community boards and then to the executive committees of each board. Feedback from each stage was documented, addressed, and shared. HHI made revisions based on collective input, including the details of the launch event being planned to introduce the artwork and the wording of outreach and marketing materials. Updates were consistently shared with both internal and external participants to maintain transparency and trust.
Throughout these interactions and presentations, Trace continued to generate opportunities for shared remembering, and in doing so, these memories shaped the work. In one example, HHI team members recall how Harlem-based community members told stories about leaders and community members who had taken up the responsibilities of community care in unique and important ways during the COVID-19 pandemic. From this, the partners determined that the launch of Trace should recognize and celebrate the work of these individuals. To actualize this, HHI made requests of local elected officials to issue proclamations to honor a small collection of people who had taken on these roles at the launch event.
The Council of Elders model thus fostered multiple forms of leadership, allowed input to move across sectors, and ensured that decisions reflected lived experience, institutional knowledge, and community values. As the event drew closer, HHI’s staff created a web-based invitation for the launch event and a cover email that explained the artwork and welcomed people “for an evening of reflection and remembrance” that would also “honor essential workers” and “individuals from the community who provided invaluable support during the pandemic”. This invitation was shared with partners far and wide, including the local community boards, the CUNY SPH Foundation, and through channels such as HHI’s newsletter, several social media platforms, and multiple personal invitations. The web-based nature of the invitation made it easy for people to share it with others.


Fruition
After 10 months of preparation, on May 28, 2025, despite the pouring rain, over 100 people gathered for the unveiling of Trace in the HHI storefront at CUNY SPH. The launch event reflected the intentional diversity of the partnerships and planning, with a cross-section of Harlem and CUNY SPH present in one room. Partners, elected officials, university personnel, and other attendees represented a range of generational, cultural, and professional backgrounds.
Practices of shared remembering formed the heart of the event. For some, this process began at the wall where Trace was printed, where greeters and wall text helped visitors understand how to interact with Trace, as it waited to be called forth through touch. For others, it began in conversations that took place around the room, shaped as they were by the imprint of the early pandemic period and the supportive ambiance of the room, like the comforting smell of Caribbean food catered by one of our own, a lifelong Harlemite; tissue packets inscribed with the tender reminder, “Just Breathe”; and QR codes sharing mental health resources. And for still others, shared remembering began with the welcome offered by Nyssa Chow in her remarks. She began with the importance of remembering as a balm: “There are names for Stars and Gods that we are not taught in high school, but our grandmothers know them. There are reasons that men in chain gangs in the South used to sing work songs to each other, and why, in times of trouble, Caribbean people go to the sea. Remembering as medicine has a long history. They knew that forgetting is the disaster. And because supremacy requires forgetting, we have a duty to remember—to become an archive for each other.” She closed with this invitation: “As an antidote to supremacy’s forgetting, I propose remembering as medicine. Choose to remember that, like the people memorialized here, we carry worlds, that we have dreams that exceed the political imagination of policies, imaginations enormous with means for a better world than this one, and hopes for our children that outlive the span of a single life. We are an archive of this.”
As Chow spoke to those gathered, attendees responded with a range of verbal and nonverbal responses, from silent nods to energetic exclamations of “Àṣẹ” (an Afro-diasporic practice of call and response), lifting the energy of the space. The invitation to participate was so alive in the room that one government official, Manhattan Deputy Borough President Keisha Sutton-James, felt compelled to step forward and take on a larger role in the moment. Initially, Sutton-James had been invited simply to present official citations to the honorees on behalf of the Borough President, but she found herself called to shift her role spontaneously. “What I experienced in that room was something deeper. The energy, the memories, the reverence for the essential workers, it moved me. I felt called to help hold the space and guide the moment so the community voices in that room could be fully heard.” As a result, she began guiding the presentation portion of the program, effectively becoming the moderator and master of ceremonies for that part of the evening.
With the overwhelming turnout of community members, the artwork’s heat-sensitive text slowly revealed itself before many had even laid hands on the wall. Unexpectedly, this collective warmth made visible all of the memories of the piece simultaneously.

Sustainability
Realizing the vision for Trace at CUNY SPH meant continuously involving the local community as the primary interest holders. Toward this goal, a team of graduate students[6] led by Emma Tsui and Arielsela Holdbrook-Smith designed materials to support engagement with the artwork and consider its potential uses. They developed 1) a Resource Guide to introduce the artwork and offer guidance for interacting with Trace, as well as mental health and social support resources that honor the artwork’s themes, and 2) an Engagement Toolkit with introductory slides and simple ways of integrating Trace into future events taking place in the space (e.g., reflection activities and discussion questions) (See Appendix). The team also created a brief experience survey for attendees to complete at the launch event and invited them to be interviewed about their experience with the artwork and suggestions for integrating it into community life. After completing these interviews, the team further developed and refined the Resource Guide and Engagement Toolkit to incorporate this feedback.
Discussion
Strengths and Challenges of CRRG Space-Making
The participation in the launch event and the processes leading up to it speak to the deep desire for and the meaning of CRRG spaces. We argue that collective grieving and remembrance practices are vital yet missing components of participatory dissemination, particularly when it centers on topics that might be attached to community grief and loss, which may encompass many types of public health issues.
Nyssa Chow has referred to encounters with Trace as “shifting the permissions of what is possible.” To interact with Trace is to be welcomed as a whole, embodied person, encountering glimpses of other people and their loved ones at the wall. It requires physical presence. The workers represented in Trace are not catalogued as statistics, as we typically might present public health data or tally harm. We cannot make sense of Trace with our brains alone. Trace activates our concurrent multisensory personal and professional experiences of the pandemic. Attendees at the launch event spoke about the experience of feeling a lost loved one’s presence at the wall, about the artwork being “moving” and “impactful”, and about the sense of “interconnectivity” that some took away from it. While touching the wall, the reverberations of policies, politics, professional practices, and choices were present. But these were not the only lenses through which we could see the people represented there. As attendees engaged with the artwork and each other at the launch event, the usual importance placed on titles and organizations was diminished. The connectedness present in the CRRG space was a direct juxtaposition to the disconnection and loneliness that defined many people’s COVID-19 experiences.
While seeking to build a space where people made differently vulnerable during the COVID-19 pandemic could come together, we attended to power and privilege throughout. Power operated across multiple levels: institutional partners initially controlled space, funds, and approval; academic partners initially exerted influence over language used and the conceptualization of goals; the artist controlled experiential and aesthetic dimensions of the work; and community members came to exert strong influence over relevance and meaning. Trace’s participatory structure thus sought to redistribute interpretive authority through iterative co-creation and repeated invitations to fill gaps identified by participants.
As a result, using practices of shared remembering and the co-created environment for collective grief, participants were able to “position themselves as affected,” something that local leaders, community members, and professionals, especially, are rarely able to do. By naming “beacons of light” (those recognized through proclamations) and acknowledging those lost, the space drew on Black and Brown rituals of remembrance and gathering to foster communal resilience. The event thus became an opportunity for catharsis, closure, and joyful reclamation. Since the launch, we have learned that Trace has inspired the idea for another memorial, this time outdoors, hosted by a different organization and centered on different orientations to this experience. We see this as further evidence of the need for these “spaces to exhale” and engage in collective remembrance and reciprocal vulnerability.
We also see two broader challenges to sustaining and growing the kinds of deeply relational, memory-centered, place-based CCRG spaces in public health. The first of these is the resistance to the importance of memory and history in the often “ahistoric” (Scally & Womack, 2004) practice of public health. While public memory work on issues relevant to the field has grown in recent years (Goggins, 2024), such as the removal of the J. Marion Sims statue and the work of Marked by COVID (Marked By Covid, n.d.), public health practitioners typically see their work as urgently forward-facing, more focused on anticipating the next public health emergency than healing and learning from the past. We see encountering these histories in ways that celebrate the “doers” and attend to how they animate the present and future, as critical to the trust-building that can make public health efforts more effective. With models like Trace, we hope that the field will continue to explore and expand public memory work and opportunities for shared remembering toward public health goals.
Second, we observe that relational place-based work in public health is increasingly short-term, project-based, and outcome-driven (Greene et al., 2025; Rong et al., 2023), and that resources for this kind of work are extremely limited. This emphasis drives transactional relationships rather than sustaining transformational ones. Maintaining active space-making practices like those we describe here will require new strategies to support relationships and make in-person gatherings both meaningful and frequent enough to keep engagement alive. In this paper, we argue that shared remembering is a powerful strategy in this toolkit. But creating these gatherings is resource-dependent—the most valuable resource being staff time—and requires institutions and funders to place intrinsic value on these relationships and practices, as opposed to conceptualizing them as optional, add-on activities (Adsul et al., 2024; Sanchez-Youngman et al., 2025; Wallerstein et al., 2023). This is made all the more challenging by the current depleted funding environment for community-focused public health.
These conditions raise broader questions: What funding models could sustain CCRG spaces over time? How might institutions value, invest in, and support through coordination, policies, procedures, and funding the community-centered relational and maintenance work that these spaces depend on? And how can partnerships adapt to preserve openness and accessibility when resources tighten (Fleming et al., 2022; Greene et al., 2025; Sanchez-Youngman et al., 2025)? Even in lean times, the social networks mobilized by the Harlem Health Initiative, the NYC Preparedness & Recovery Institute, and Trace offer lessons about resilience. We continue to watch how these relationships might shape future public health work, both intentionally and unexpectedly.
How CRRG Space-Making Can Support Participatory Research Dissemination
We see the co-creation of CRRG spaces as critical to integrate into public health practice generally, but we see particular benefits of CRRG spaces for making research dissemination participatory, meaningful, and perhaps healing. As our story hopefully suggests, these spaces are as much social spaces as they are physical spaces. The ongoing invitations and connections that build these spaces respond to longstanding concerns in the community and academic partnership literature that power must be named, examined, and addressed in real time, particularly in equity-centered work (Fleming et al., 2022; Sanchez-Youngman et al., 2025).
To embark on CRRG space-making, we encourage individuals engaged in participatory research to begin collaborative discussions early in the process, guided by the following questions:
-
What is the historical context of the focal public health issue?
-
What harms occurred? Where was trust across groups lost?
-
What and who promoted resilience? Where was trust across groups gained?
-
If it is an emergent issue (e.g., a novel virus or an environmental issue that has not previously affected this place), what similar issues has the local community grappled with?
-
-
What kinds of social spaces are needed to disseminate research on this topic with the potential for healing and reclamation?
-
What do people most vulnerable to the focal issue need or desire beyond information and public health action?
-
How do we create space to meet these needs/desires?
-
How do we make space for collective grieving?
-
How do we recognize the work of vulnerable people?
-
-
What role might shared remembering play in building relationships across differential vulnerability?
-
What kinds of memorials might exist or be created locally to anchor and generate shared remembering?
-
What kinds of storytelling practices might support shared remembering, whether informal or formal?
-
How might power shape where and how shared remembering can and should take place?
-
-
How might using the Council of Elders approach or similar methods help to ensure wide participation, cultural relevance, and recognition of accomplishments?
-
Which organizations have earned a deep trust of community members through years of consistent presence, especially during moments of crisis, loss, or collective struggle?
-
How can these organizations be engaged not just as partners but as co-designers and stewards of the space, ensuring the process reflects community values, culture, and lived experience?
-
How can community members and local “beacons of light” best be identified and acknowledged?
-
How can other sectors participate in and elevate the emergent CRRG space?
-
As these questions suggest, one important consideration is that CRRG space-making of this kind requires the ability to engage organizations like the Harlem Health Initiative and others involved in the Council of Elders outreach to guide the process and anchor it in local values. It is critical to identify grassroots groups, faith communities, cultural institutions, and neighborhood organizations that already serve as safe gathering spaces where people share stories, support one another, and process community experiences, if they exist.
We also encourage community-academic partnerships to consider the role of art in this kind of space-making. While we can imagine a similar process taking place without an artwork at its center, we believe that gathering around art, in particular, may have unique community-building effects that can support research dissemination moving toward community-centered action. Research indicates that integration of the arts into community development can engage people who otherwise might not be involved (Catalani et al., 2022; Sonke et al., 2019), and we saw this powerfully demonstrated in our project. Art forms that invite shared remembering and collective storytelling, whether through memorials, murals, or performance, may be especially powerful tools for relationship-building across groups (Fullilove & Fullilove, 1999). Carnival traditions offer one model. They combine costume, music, and dance into a participatory experience where everyone becomes both performer and audience. Public health initiatives could draw on this approach, designing dissemination events that feel celebratory rather than didactic, communal rather than hierarchical (Minkler, 2005). Graffiti and street art provide another model. These forms claim space in the public realm and signal local ownership of narratives. A mural co-created by community members could serve as a visible record of the past, as well as of health priorities and accomplishments, accessible long after a research report has been filed away. In this way, dissemination becomes less a unidirectional transfer of findings and more a process of collective interpretation. As an example, a dissemination event on neighborhood asthma rates or an infectious disease outbreak could include participatory storytelling or sensory elements that connect quantitative results to community memories and strengths. These modalities expand access and deepen understanding, allowing data to be encountered not only intellectually but also through the body, emotionally, and collectively.
Conclusion
The installation of Trace within the Harlem Health Initiative space demonstrates how an environment grounded in remembrance, relationality, and care can be collectively created, and inspires us to think about what such a space can do for participatory dissemination. Sharing research findings in the context of a CRRG space has the potential to expand access and deepen understanding, allowing data to be encountered not only intellectually but also emotionally and collectively. The work of Trace also highlights a broader challenge: how institutions can assume responsibility for maintaining such infrastructures after the initial project concludes. Participatory dissemination requires not only creativity and trust but also investments in people and places. Sustaining this work means recognizing care, continuity, and relationship-building as essential forms of public health practice.

Acknowledgments
The installation would not have been possible without the support of team members throughout the university, assisting in the coordination of logistics required in maintaining a space conducive for the piece to thrive and navigating the systems involved with art acquisition. Kamrun Nahar, NYC Preparedness and Recovery Institute, and Holly Farkas, Office of Government Affairs, provided vital support during the installation and article-writing processes. We are also grateful to Leslie Diuguid, Makaio Johnson, Naia Bautista, and Shannon Stovall, who brought Trace to life on 125th Street, and to MPH students Araceli Campos and Ramla Sahib Din, who worked with dedication to help create the Resource Guide and Engagement Toolkit. We extend deep gratitude to the elected officials who issued proclamations and citations at the Trace launch event. Finally, we are humbled by the numerous communities and individuals who have embraced the artwork and the project, making it an integral part of their lives.