

Introduction
Study Background
Women of color and lesbian, gay, bisexual, pansexual, and queer women (LGB+ women) experience alarming inequities in perinatal health and healthcare compared to white and heterosexual women (Crear-Perry et al., 2021; Januwalla et al., 2019), driven by structural factors including medical racism, heterosexism, and poorer access to respectful perinatal care (Crear-Perry et al., 2021; Goldberg et al., 2017; Gregg, 2018; Griggs et al., 2021; Januwalla et al., 2019; Njoku et al., 2023; Permezel et al., 2023). Majority of pregnant LGB+ women identify as bisexual (Gonzales et al., 2019), and nationally representative data reveals that more women of color identify as bisexual (35%) than heterosexual (25%) (Beach et al., 2018; Movement Advancement Project, 2016). Despite comprising a significant proportion of the childbearing population and documented perinatal disparities among women of color and LGB+ women, the priorities and experiences of bisexual women of color remain largely invisible within obstetric literature and perinatal health equity initiatives. To begin addressing this gap, our team led a two-year community-engaged study to examine bisexual women of color’s perinatal healthcare experiences. We led in-depth interviews with 15 bisexual women of color about their perinatal care priorities, desires, and needs and generated community-directed recommendations for advancing reproductive justice and perinatal health equity. In this manuscript, we describe the participatory processes undertaken to plan an arts-based multimedia dissemination event aimed at sharing findings from our interviews with study participants, community members, birth workers, and healthcare professionals.
Community-engaged research and participatory dissemination
Participatory research is an umbrella term that describes the collective of research designs, methods, and frameworks used in partnership with communities to enact change (Cargo & Mercer, 2008) . One of the participatory approaches frequently used across the public health field is community-engagement (Ahmed & Palermo, 2010; Key et al., 2019). Community-engaged research emphasizes equitable collaboration with community members throughout each step of the project lifecycle to center community research priorities and co-create solutions that advance health justice (Holden et al., 2015; Holzer et al., 2014; Vaughn & Jacquez, 2020). This approach disrupts traditional research dynamics by prioritizing power sharing between community partners and research teams, honoring community wisdom and leadership, and supporting long-term community capacity building for research (Allen et al., 2021). Meaningful community engagement holds the potential to generate research that is trustworthy and responsive to community needs (Thorpe & Islam, 2025)—both of which are central to advancing perinatal health equity and reproductive justice (Davis et al., 2022; McGlothen-Bell et al., 2022).
Participatory dissemination is a critical step in community-engaged research, as equitable research approaches should promote partnership in knowledge generation and action (Wallerstein et al., 2017). Community engagement in the dissemination process upholds ethical research principles (Chen et al., 2010), counters the damaging impacts of extractive “helicopter research” (McIntosh et al., 2023) and “health equity tourism”(Lett et al., 2022), and accelerates progress towards systems-level change (Gollust et al., 2025; Purvis et al., 2021). By co-developing materials with community partners and collaboratively sharing findings through accessible mediums, participatory dissemination is recognized as a bridge to close gaps between research and practice (Minkler & Salvatore, 2012). Despite the increased emphasis on the importance of participatory dissemination and co-design processes, these practices are still inconsistently implemented across health research, with many researchers spending an insufficient amount of time on dissemination planning (Cunningham-Erves et al., 2020; Gollust et al., 2025) . Additionally, while much of the literature on participatory dissemination focuses on returning results to participants, less attention has been brought to methods for co-designing dissemination activities that reach a range of audiences who can benefit from the work (Bodison et al., 2015; Concannon et al., 2012; Gollust et al., 2025). Our article addresses these gaps in the literature by outlining actionable techniques for planning participatory dissemination activities that reach diverse audiences. We share strategies that facilitated community-led decision-making throughout the dissemination process, which can be adopted by researchers, community members, and other practitioners who facilitate and participate in community-engaged projects. Finally, despite growing interest in art-based dissemination methods, little literature exists on how these methods work in practice, including specific steps for planning and implementing this methodology with community members (Ball et al., 2021). Accordingly, our manuscript makes a novel contribution to arts-based dissemination literature by detailing our co-design process, which can guide other teams in utilizing this methodology.
Methods
THRIVE steering committee
This project was led in partnership with THRIVE, a virtual steering committee established by the Principal Investigator (DW) in the Fall of 2023. She is a Black woman with over a decade of experience working alongside the BIPOC LGBTQ+ community in health equity contexts. THRIVE is comprised of eight members across the Pacific Northwest who hold personal and/or professional experiences in relation to the study population and the research topic. Our group includes representation from birth workers, community leaders and activists, parents, and community-based perinatal healthcare professionals. Majority of members identify as bisexual/Queer and BIPOC (Black, Indigenous, People of Color). From Fall 2023 to Spring 2025, THRIVE convened virtually eight times each study year for 90 minutes to lead study decision-making, engage in co-design processes, and collaborate across each phase of the research lifecycle, including study design, participant recruitment, data collection, analysis and interpretation, and dissemination. A subset of members also attended small-group working meetings between these convenings. All members received an honorarium in appreciation of their time throughout the study. In line with equitable community-engagement principles, five THRIVE members are co-authors on this paper.
Framework guiding participatory dissemination
Our project is guided by the Reproductive Justice Framework, a Black feminist framework rooted in tenets of intersectionality and human rights (L. Ross & Solinger, 2017). Reproductive Justice promotes three core rights, including a person’s right to: (1) decide to have a child and determine the conditions of their birth, (2) decide not to have a child and prevent or end a pregnancy, and (3) parent children in safe and healthy environments where families can thrive (Julian et al., 2020; L. J. Ross, 2017; L. Ross & Solinger, 2017). Central to Reproductive Justice is the understanding that intersectional systems of power and oppression threaten bodily autonomy and reproductive self-determination (L. J. Ross, 2017). Therefore, justice-based change-making cannot be achieved across the perinatal health field without critiquing and addressing the structural drivers of inequity that shape people’s reproductive lives, decisions, and experiences (e.g., racism, sexism, heterosexism, and binegativity) (Morison, 2021). This recognition is especially crucial as social narratives frequently place blame on women of color when they experience adverse perinatal health outcomes, while ignoring the contexts and conditions in which they maintain their perinatal wellbeing (Scott et al., 2019). Reproductive Justice disrupts these detrimental, deficit-based narratives by illuminating the root causes of perinatal health inequity and grounding community wisdom in strategies to transform perinatal healthcare and improve perinatal health outcomes (Ertl et al., 2024; Julian et al., 2020; L. J. Ross, 2017).
Across our dissemination planning and co-creation process, we used three approaches from the Reproductive Justice Framework to guide our work (Table 1). First, Reproductive Justice offered us a lens for interrogating multidimensional power dynamics and reproductive restraints that impact the perinatal health and healthcare experiences of bisexual women of color (RJ approach 1). For instance, many of participants’ experiences called attention to healthcare policies and practices that perpetuate inequitable care. As we created our pieces, Reproductive Justice provided a framework to examine the overlapping systems of power entrenched within these policies and practices, allowing us highlight to the root causes of perinatal healthcare inequities among bisexual women of color. Second, during our dissemination planning convenings, we determined that one of our event goals was to encourage community dialogue around the responsibility of healthcare systems in fostering safe and equitable care across the perinatal continuum (RJ approach 2). In doing so, we intended to promote reflection on anti-racist accountability among birth workers and healthcare professionals who play a significant role in redressing perinatal health inequities (Menard et al., 2015), directly countering the pervasive nature of mother blame. Finally, we were cognizant of how crisis and trauma-based narratives have largely dominated social discourse around women of color’s perinatal experiences. While it is undoubtedly important to understand and address birthing trauma, solely focusing on disparities and adverse experiences masks the full spectrum of bisexual women of color’s lives, “erasing stories of joy, resilience, and thriving (Opara & Elmi, 2025).” During our dissemination planning meetings, we prioritized interweaving strengths-based narratives from participants in our pieces, highlighting themes of empowerment, healing, community power, affirmation, and autonomy (RJ approach 3). Doing so resisted singular narratives that limit holistic representations of the reproductive lives of bisexual women of color.
Participatory dissemination planning
Large group convenings
a. Co-developing a guiding vision
To begin planning for dissemination, we first reflected on our dissemination priorities within our large group convening. DW posed two questions to facilitate this discussion: 1) What factors are most critical in shaping our vision for sharing back our findings, and 2) What impact do we hope our dissemination will have? After considering these questions independently and writing down our thoughts, each of us shared our responses with the group and identified areas of overlap across our perspectives. Three core priorities came forward from this discussion: 1) sharing information that is accessible, understandable, timely, and disrupts traditional power dynamics in research (RJ approach 1), 2) ensuring information reaches families and bisexual women of color with children, given our perinatal health focus, and 3) promoting dialogue and engagement through our dissemination methods (RJ approach 2). Situating these priorities within the Reproductive Justice Framework helped us establish a guiding vision for our dissemination methods, serving as a roadmap for future planning discussions.
b. Idea generation
During our next large group convening, we utilized a virtual collaboration board to map our dissemination methods through two brainstorming rounds. In the first round, we generated initial ideas around our dissemination audience and medium. Given the erasure of bisexual women of color in perinatal health research, we wanted our findings to reach interview participants as well as bisexual women of color in the community to honor their experiences and cultivate space for affirmative community-building. We also desired reaching birth workers and healthcare professionals, as both groups work directly with bisexual women of color across the perinatal continuum and are critical to advancing equitable care experiences (RJ approach 2). Finally, we sought to engage with local community members, acknowledging the importance of supporting community power building and advocacy in the pursuit of reproductive justice (RJ approach 3). When generating ideas around our dissemination medium, we thoughtfully considered what platform would reach all of our priority audiences. We brainstormed the advantages and disadvantages of several mediums (Table 2) and decided that an arts-based multimedia event was most closely aligned with our vision and Reproductive Justice approaches.
Arts-based research is a growing methodology across the social sciences that is rooted in qualitative inquiry (Fraser & Sayah, 2011). The arts are a powerful communication tool that can improve public engagement with science, center perspectives that often fall on the margins, and promote dialogue that empowers communities to respond to research (Ball et al., 2021; Paat et al., 2025). Arts-based dissemination methods move beyond traditional and textual accounts of research outcomes, challenging assumptions about scientific ways of knowing (Finley, 2008). This dissemination method democratizes research, relocating social inquiry to everyday places and events, rather than confining it solely to inaccessible academic spaces (Finley, 2008; Foster, 2012). Approaches to arts-based dissemination are vast, and may include art installations, poetry, photography, drama, and film (Ball et al., 2021). Therefore, research art engages the senses, emotions, and imagination to address social inequities (Finley, 2008).
Researchers frequently use arts-based dissemination to engage a broad and diverse audience and to increase community research impact (Ball et al., 2021). Our team chose this methodology for similar reasons, as we intended to reach three distinct audience groups and enhance opportunities for communities to respond to our work. In the healthcare field in particular, artistic endeavors are often used to articulate the embodied experiences of patients with the goal of influencing clinical practice (Fraser & Sayah, 2011; Lapum et al., 2014). Likewise, we aimed to share recommendations for transforming the future of perinatal healthcare through our artistic works, grounding each piece in the wisdom and embodied knowledge of bisexual women of color. Participatory in nature, arts-based methods also encourage the co-production of creative pieces among researchers, community members, and artists (Byrne et al., 2018; Rydzik et al., 2013), aligning with our research values.
In our second brainstorming round, we brought forward ideas regarding the core details of the multimedia event, including the venue, program structure and types of pieces to be shared, messaging, and a planning and implementation timeline (Table 3). We reflected on each question in Table 3 independently and discussed our perspectives with the group. Afterwards, we shared which ideas resonated the most to start crystallizing our event outline. We temporarily tabled ideas that required further examination; for instance, our decision-making regarding venues was contingent on availability and cost and therefore was determined later in our planning process.
Small work group sessions
a. Collective decision-making through an iterative, circular discussion process
While all THRIVE members were involved in the brainstorming process during the large group convenings, those of us who intended to create and share pieces for the event (CH, EK, KM, DJ, FG) gathered at two virtual working sessions (facilitated by DW) for final decision-making on the event outline using an iterative, circular discussion approach to harness our collective wisdom and promote shared understanding. Our discussion process consisted of five phases: idea formation, idea filtering, elaborating, refining, and building consensus. Below, we provide an example of how we implemented this method in our working sessions (Table 4).
We planned to incorporate an audience activity at the event to foster engagement and promote audience dialogue (RJ approach 2). During the idea formation phase of our discussion, several options emerged, including the creation of a community poem, a participant quote gallery, shadow art, and yarn art. During the idea filtering phase, we assessed the feasibility of each option, eliminating ideas that would be challenging to implement within our event space. After narrowing down options to yarn art and a quote gallery featuring participants’ visions for joyful and justice-based perinatal healthcare (RJ approach 3), we reflected on how to merge these activities to encourage creative engagement with participants’ quotes. During the elaboration phase, several of us suggested drawing inspiration from latch hook crafting, a beginner-friendly art method that involves threading yarn through a grid-like canvas to create an image. After developing synergy around this idea, we refined the activity to ensure it would be accessible and open to audience members of all ages, in line with our guiding vision. In the consensus-building stage, we reviewed notes from our previous discussions and reached a collective agreement on the final elements of the activity.
b. Co-creating art pieces
Our small group work sessions also offered focused collaboration time on our pieces and an accountability method for moving our work forward. In advance of the first session, we reviewed themed data and exemplary quotes from the interviews to begin shaping our pieces. Upon gathering, we shared which themes and quotes felt most aligned with our artistic visions, intending to find a balance between pieces that focused on intersectional systems of power (RJ approach 1) and those centered on intersectional strengths and assets (RJ approach 3). This discussion helped us determine how participant narratives would be captured across our art and who would focus on specific elements of each story.
One of the core questions we considered during our sessions was how we hoped audience members would feel at our event, as art-based dissemination methods can support the processing of emotions (Dadich et al., 2025). This question helped guide the creative direction of our pieces. For example, CH’s piece highlighted forms of disrespect that participants experienced during their perinatal care, however CH included an interactive component to the piece to offer opportunities for community healing and reclaiming power. After working on our pieces independently between sessions, we met for the second small group meeting to show our works in progress, address creative challenges and questions, and share feedback on our creative directions.
Over the course of our two-year partnership, we have developed a deep sense of relationality and trust with one another, supporting each other through resource sharing and acts of solidarity. Therefore, it was essential to us that our small group sessions also provided space for peer support regarding the emotions that arose as we created our pieces.
Dress Rehearsal
The week before our event, we held a virtual dress rehearsal to practice the flow of the program and speaking about our pieces. We finalized how each piece would be introduced and the order of the event, choosing to end on a message of hope leading into the audience activity. During this rehearsal, we also confirmed our supporting roles at the event (such as greeting guests) and reviewed the RSVP list to project our final attendance.
Participatory Dissemination Event
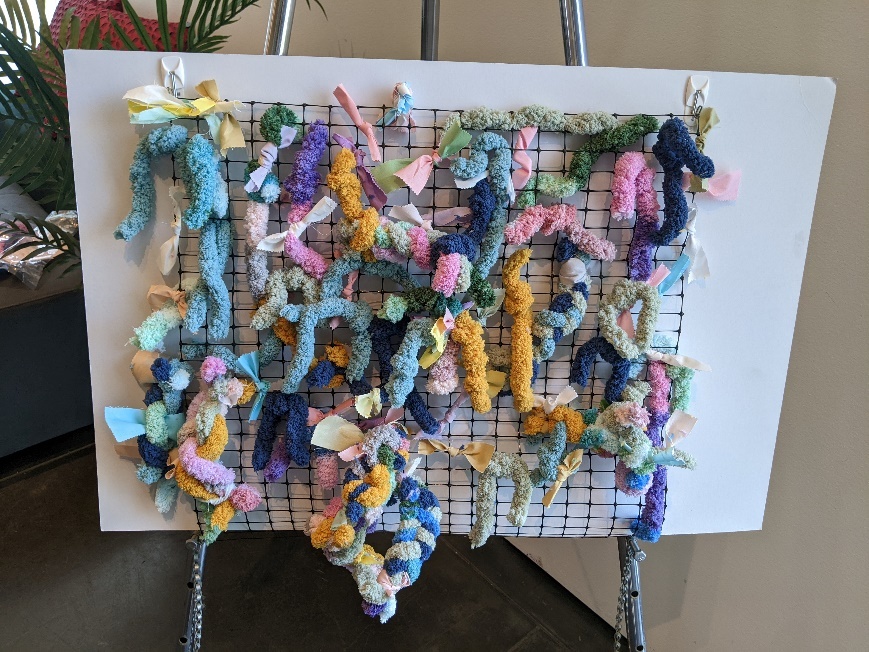
We held the multimedia event in June 2025. The event was hosted in a hybrid format online and in person at a local art museum in Washington state, reaching around 25 audience members in total, including community members, birth workers, healthcare professionals, and reproductive justice advocates. Our event began with a moment of centering through guided breathing. Over the course of the program, we featured six pieces directly informed by the narratives and quotes of our participants, including four poems, an interactive tape casting of a pregnant person, and a collection of art pieces featuring acrylic and mixed media on canvas, as well as mixed textiles and media. To close the event, we invited the audience to engage with the gallery of participant quotes centered on ways to advance reproductive justice and joy in perinatal healthcare (RJ approach 2 & 3). Audience members collected yarn from each quote board that resonated with them and threaded these pieces of yarn through a mesh canvas to create a community art piece (Image 1).

Each of us will briefly describe the title and meaning behind our piece, with images of our media included below.
“So Much for the Hippocratic Oath” by C. Hawthorne
This piece features a tape-casted sculpture of a bisexual person of color in their last trimester of pregnancy. Along their body are wounds that represent comments, expectations, and assumptions from their perinatal care team. Every wound was inspired by the collective experiences of each bisexual woman of color who shared their stories (Image 2). With this piece, we are also called to envision how accountability can and should look like within the healthcare system, as audience members were invited to write notes of hope and support to cover and “heal” the wounds.

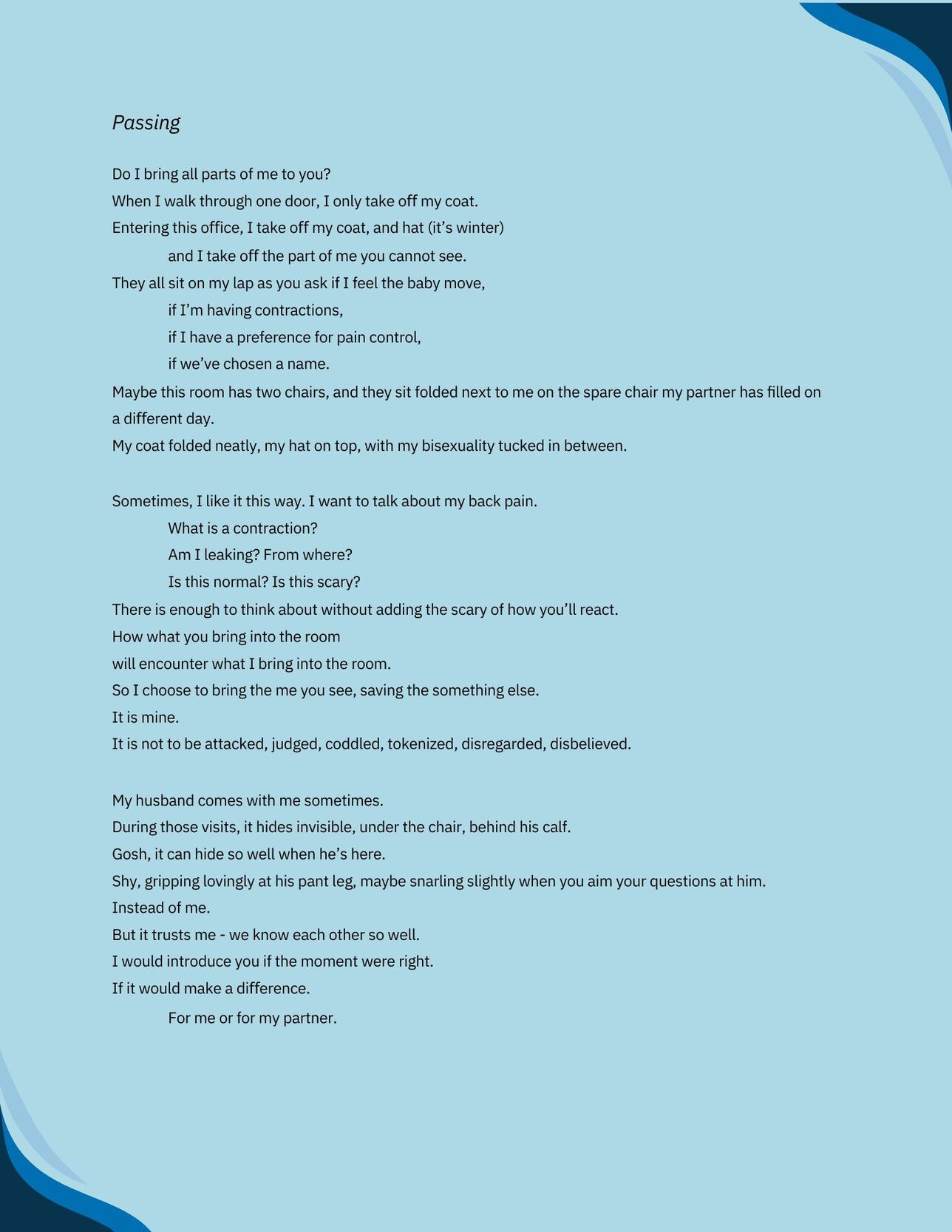
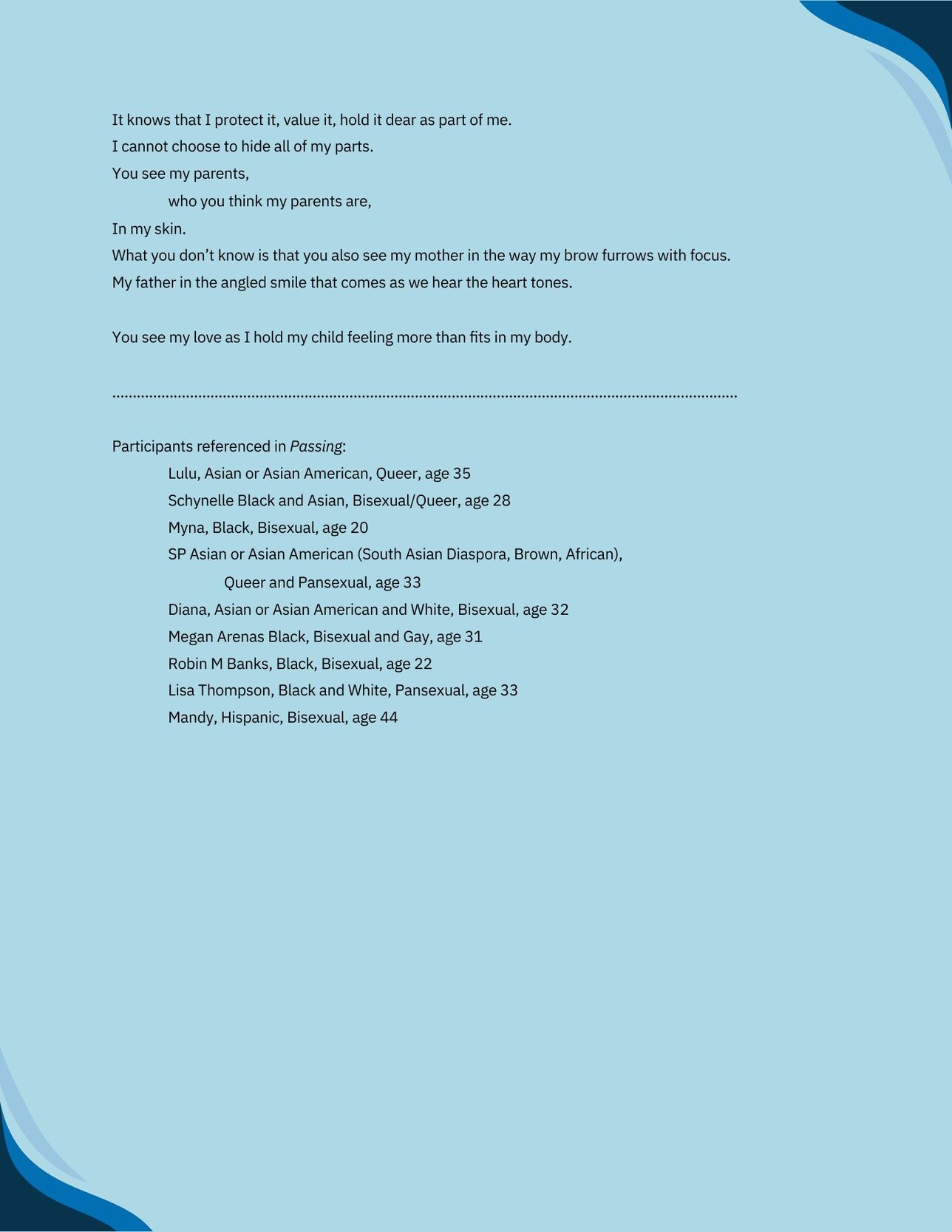
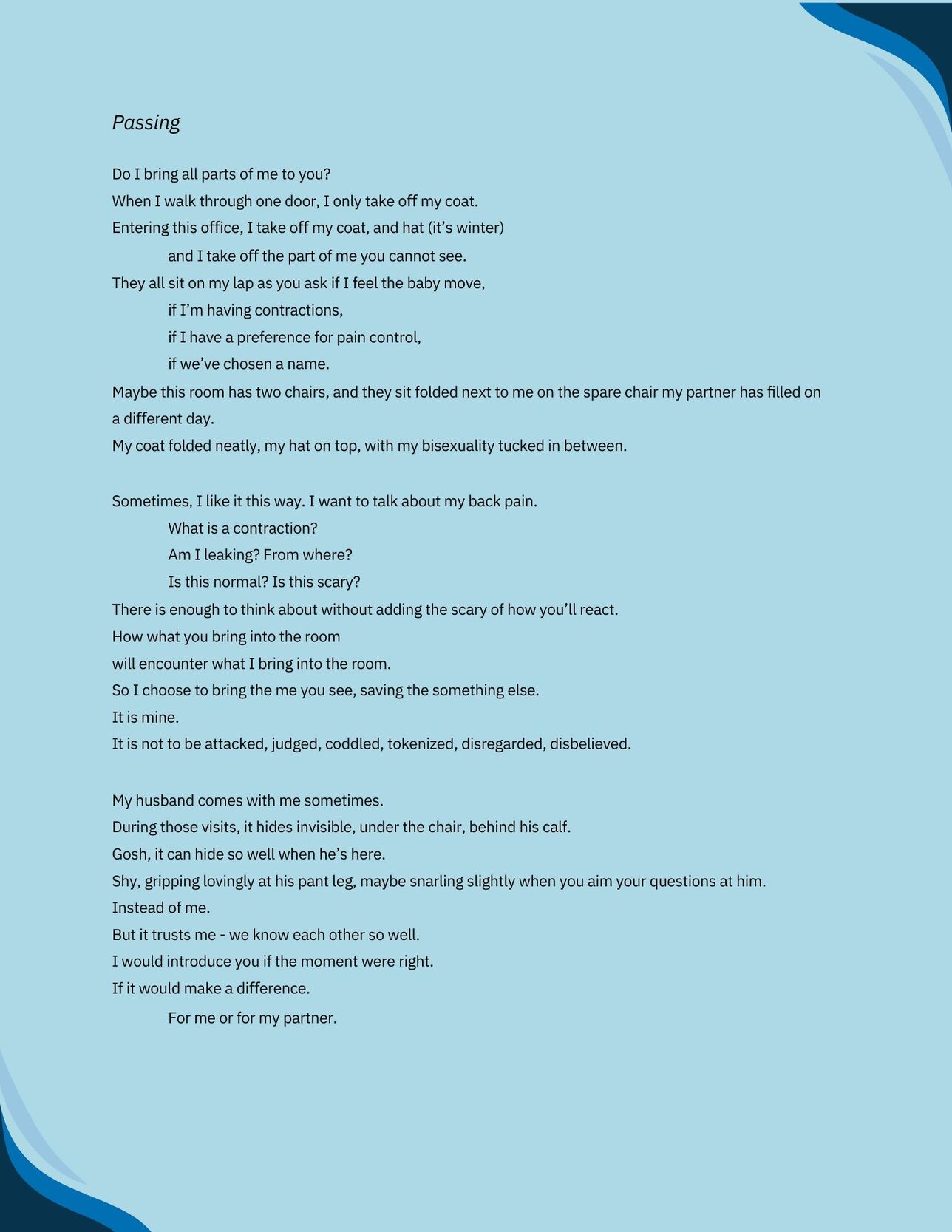
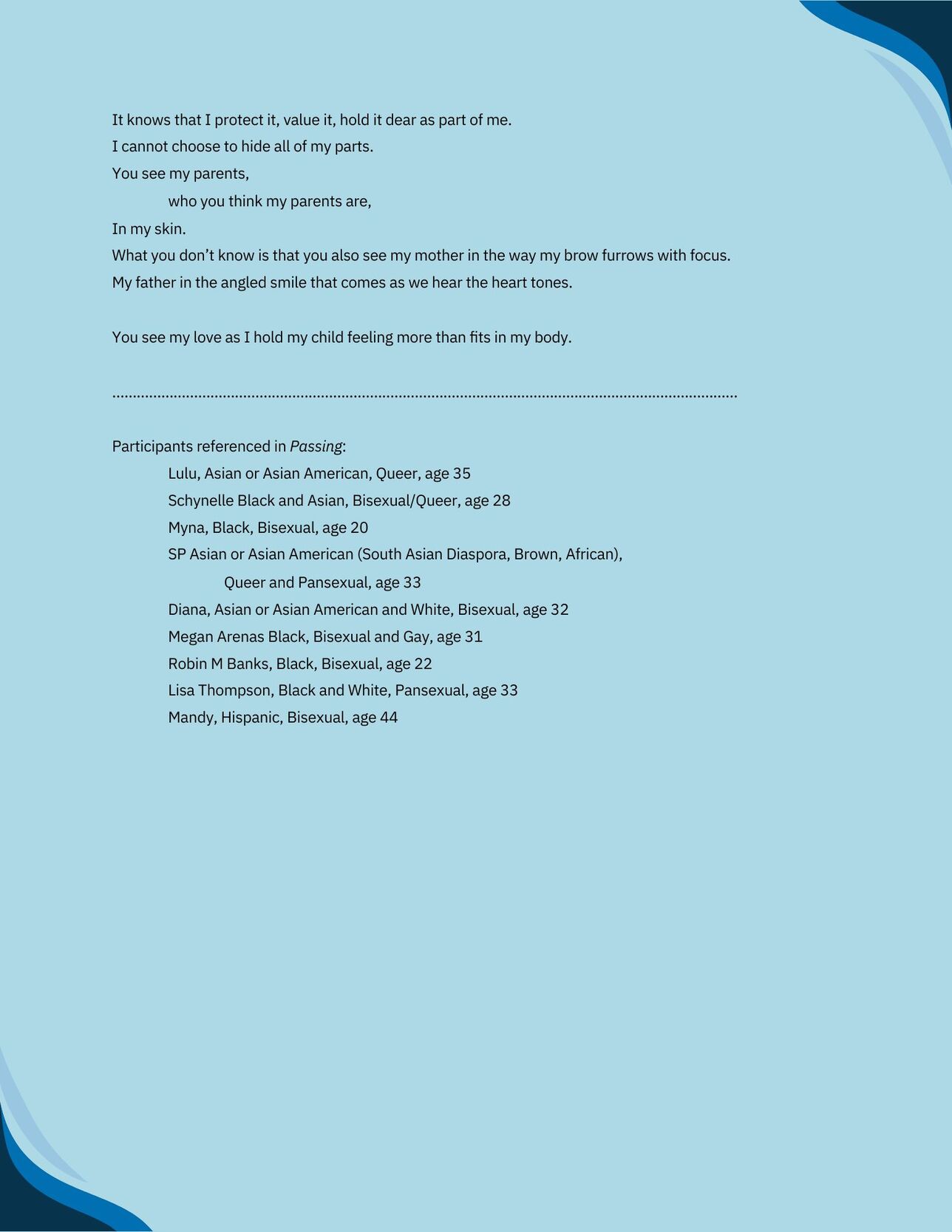
“Passing” by Elizabeth Karin
This poem (Image 3) was inspired by bisexual women of colors’ references to bisexual identity concealment, feelings of invisibility, and experiences of heteronormativity within the healthcare system. This poem captures the complexity and duality between navigating the stress of identity erasure and moments of chosen concealment as a form of protection, leaving us with the question, what does it mean to be seen? Passing was also inspired by the joy and beauty of bringing new life into the world.
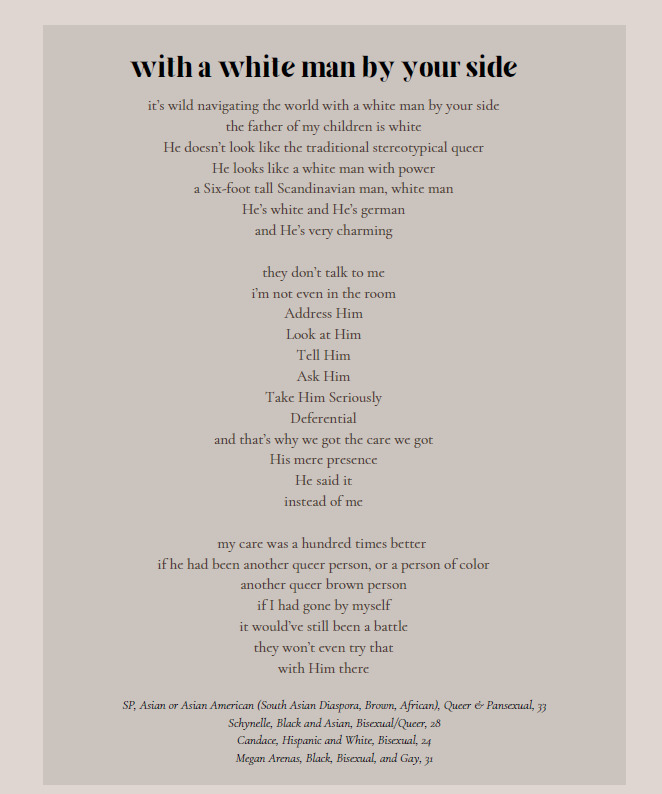
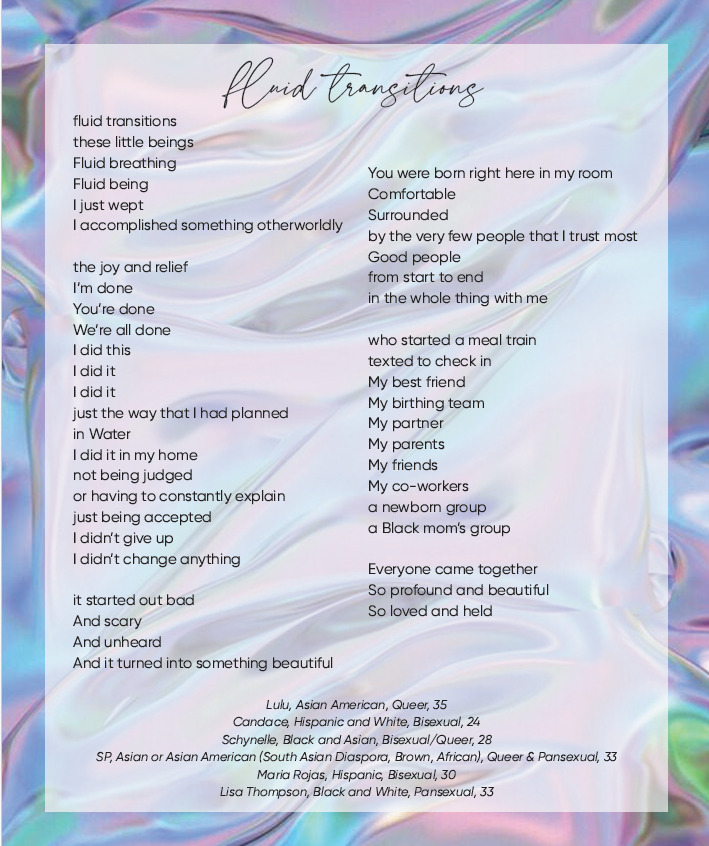
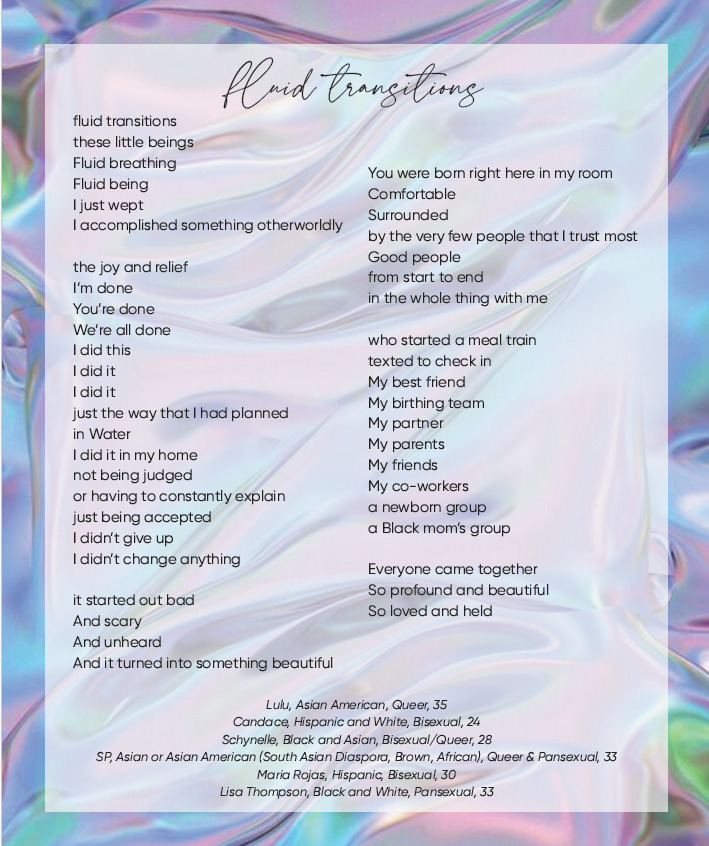
“With a white Man by Your Side” and “Fluid Transitions” by Karissa Masciel
With a white Man by Your Side (Image 4) highlights how experiences of care differed for bisexual women of color depending on who attended their perinatal appointments with them, underlying racialized binegativity and heteropatriarchy within the healthcare system. Fluid Transitions (Image 5) celebrates community, connection, and birthing joy. Both poems were created using the exact words of participants.

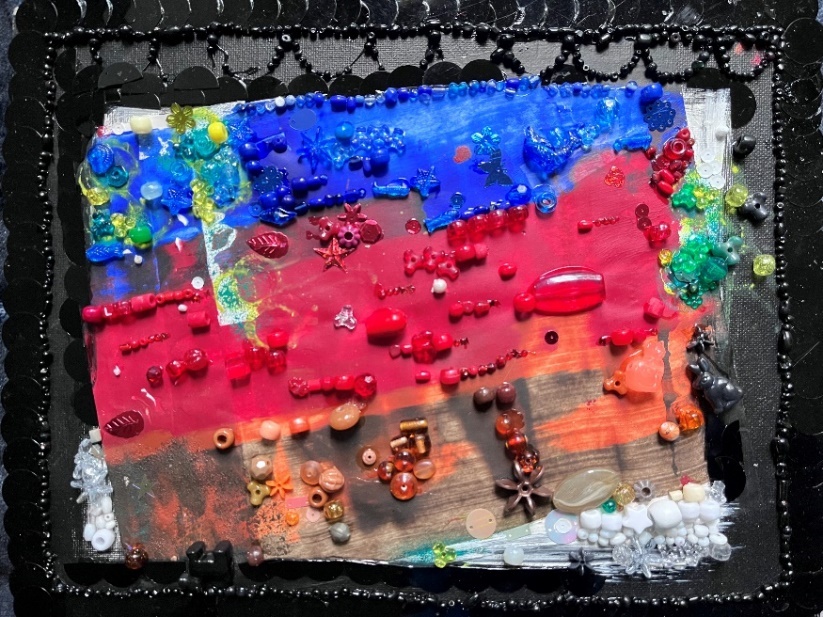
“Cycles” “Colorblind” and “Altars para Ti” by Drea Johnson
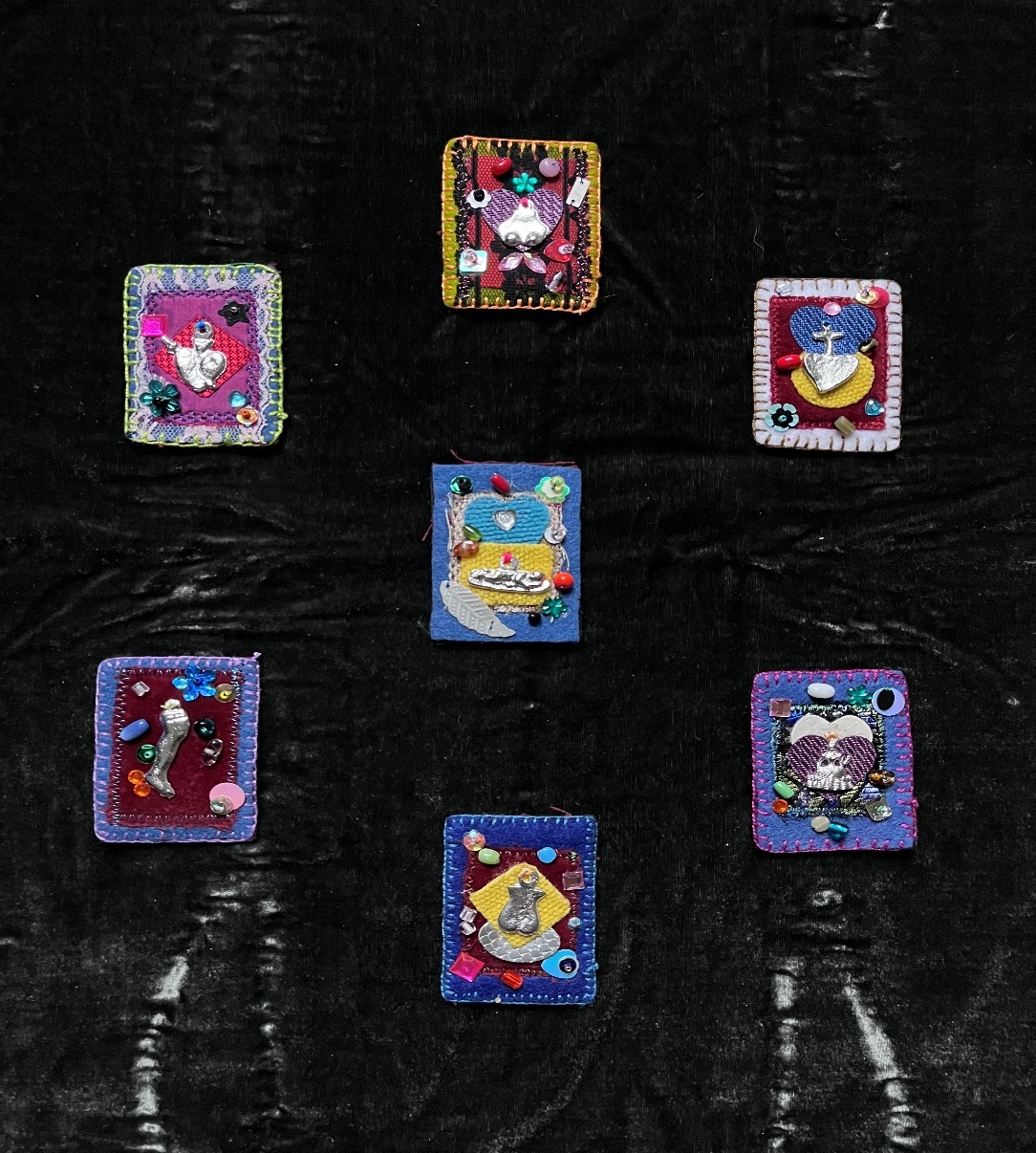
The first piece “cycles” represents bisexual women of colors’ body not feeling like their own during the perinatal continuum, highlighting the loss of body autonomy, (Image 6), the second piece "colorblind" amplifies the issue with assuming that one size perinatal care fits all (image 7), and the final piece “altars para ti” features a collection of embroidered Mexican amulets representing alters for birthing celebration, peace, prayer, or grief (image 8).


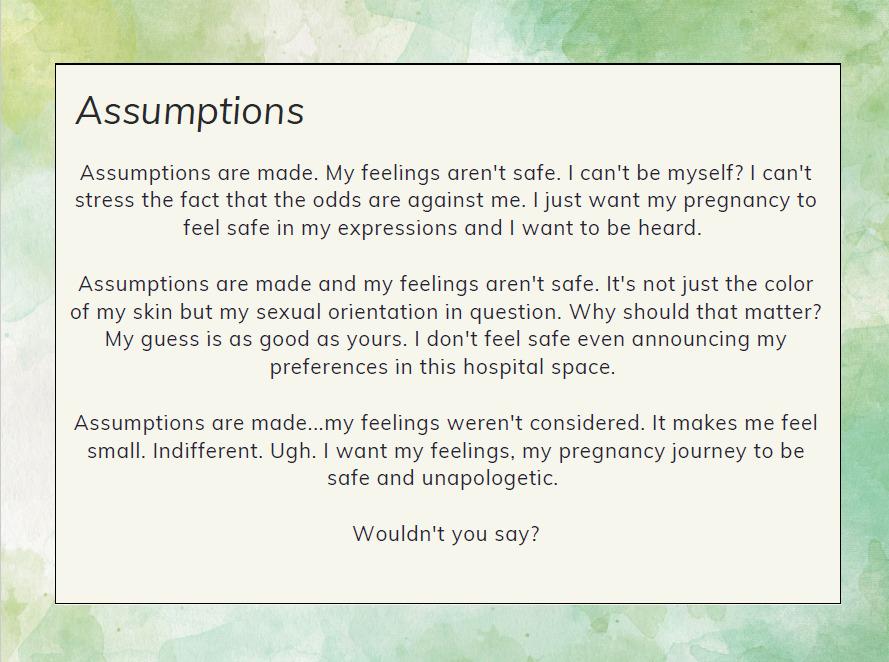
“Assumptions” by Felecia Graham
This poem (Image 9) explores how assumptions made within the perinatal healthcare system can leave bisexual women of color feeling unsafe and unheard, inviting us to consider how assumptions get in the way of birthing justice.
The event was well-received by attendees and celebrated for sharing research findings through a creative and engaging dissemination method that supported community action around perinatal health inequities. Several birth workers and healthcare professionals also expressed interest in engaging in further dialogue around the participant quote gallery with their colleagues, highlighting the power of personal narratives in driving change within the healthcare system. Attendees suggested hosting a training or workshop integrating these quotes with birth workers and healthcare professionals. This feedback was particularly meaningful given our intention to foster community dialogue about the healthcare system’s responsibility in disrupting the systems of power that perpetuate harmful perinatal healthcare experiences and outcomes (RJ approach 2).
Strengths and Limitations
Participatory dissemination through arts-based multimedia served as an effective, accessible, and innovative methodology to bring visibility to bisexual women of color’s perinatal healthcare experiences and increase critical dialogue around perinatal health equity. Further, arts-based dissemination methods are uniquely positioned to illuminate intersectional forms of oppression and outline possibilities for transformative praxis- both of which are necessary in moving towards a future of reproductive justice (Finley, 2008). Our participatory dissemination planning process has several strengths. THRIVE convenes virtually as we live in different states across the Pacific Northwest. While some may view this as a disadvantage for collaboration, implementing methods and tools such as circular discussion phases and virtual collaboration boards supported equitable decision-making and sustained engagement among our group. Given the rise in online community coalitions and committees resulting from COVID-19, future research should examine which virtual collaboration tools and strategies are most conducive to participatory research.
Starting our co-design process with a guiding vision for dissemination was also a strength because it kept us focused on working towards our collective goal and helped align our decision-making. For instance, when deciding themes to highlight in our pieces, recalling our guiding vision helped us remain accountable in rejecting deficit-based messaging. Finally, convening in both large and small group settings presented several advantages. Our large group meetings offered all THRIVE members the opportunity to drive the direction of our dissemination, while small group sessions provided focused time for event refinement, collaborative work on pieces, and social support among those implementing the event.
Our dissemination planning process also presented limitations. Due to scheduling conflicts, THRIVE members were occasionally unable to attend specific large and small group meetings. While DW often connected with members separately to share meeting notes and capture their input on decisions, we recognize that ideas and questions generated outside of the collective may differ from those that would arise in a shared space. While we began planning for dissemination six months prior to hosting our event, we still experienced time constraints throughout our collaboration. Within our large group convenings, dissemination planning was a portion of our agenda; however, we also had additional project tasks to complete during these meetings. Therefore, at times, it was challenging to balance our timing for dissemination discussions while reserving enough time for additional project components. To mitigate timing constraints, we recommend beginning dissemination planning earlier in the project lifecycle, as outlined by Gollust and colleagues (Gollust et al., 2025) and allocating dedicated time for dissemination meetings outside of regular convenings. Teams should also ensure their projects have sufficient funding to compensate community partners for attending extra meetings or rehearsals, as this is a critical component of equitable community-engaged research (Giacomozzi et al., 2025). Finally, we note that our event reached a smaller audience than intended; while we intentionally hosted our event during PRIDE month in June, we acknowledge that other LGBTQ+ community events occurred during the same timeframe, which may have shaped our attendance. Further, the venue experienced an unexpected internet disruption during the event, which impacted online attendees’ ability to join or rejoin the event. Despite these challenges, our event sparked meaningful dialogue and created opportunities for community building, critical reflection, and public health action.
Conclusion and Implications
Participatory dissemination through multimedia serves as a creative, interactive, and justice-based format to share the lived experiences of communities who are often excluded within research, including bisexual women of color. The artistic works and quote gallery from this dissemination event can be embedded within future trainings or community workshops to advance anti-racist, bisexual affirming clinical practices among healthcare professionals and birth workers. Bisexual women of color’s visions for joyful and justice-based care can also inform the development of community-oriented models of care, state-wide quality improvement directives, and accountability mechanisms within healthcare systems that foster a culture of responsibility in tracking process towards perinatal health equity.
Given expanded interest in arts-based research across the health sciences and the limited amount of literature outlining practical steps for participatory arts-based dissemination (Ball et al., 2021; Lapum et al., 2014), our manuscript can serve as a how-to guide for researchers, community members, and practitioners interested in this methodology. Further, our discussion techniques and co-design activities can be adopted by a range of audiences, supporting users in promoting equitable community engagement and decision-making throughout their projects and initiatives. Finally, this paper can inform remote collaboration efforts by offering successful partnership and dissemination planning strategies can be implemented in an online setting.
Acknowledgements
We are deeply grateful to all the members of THRIVE for their commitment to this project and work towards advancing reproductive justice. We also express gratitude to those who took part in the interviews-thank you for trusting us with your stories and bringing visibility to bisexual women of color’s experiences.
Funding
Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number 3UL1TR002319-08S1 (2023-2024). It is subject to the NIH Public Access Policy. Through acceptance of this federal funding, NIH has been given a right to make this manuscript publicly available in PubMed Central upon the Official Date of Publication, as defined by NIH. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.