

Introduction
Post-Traumatic Stress Disorder (PTSD) is a common mental health issue. Depending on study methods, 3-6% of men and 8-13% of women have had PTSD during their lifetime, over half of these during the past year (Kilpatrick et al., 2013; Lehavot et al., 2018). Thus, nearly 5 million men and more than 10 million women met criteria for PTSD during the last year. These numbers are more than twice as high among military veterans (Lehavot et al., 2018) and even higher among combat veterans (Hoge et al., 2004) compared to civilians (non-military). Assessments of the point prevalence of veterans who served in combat units in Iraq and Afghanistan range as high as 23% when data from multiple studies are combined; individual studies cite rates exceeding 50% (Fulton et al., 2015; Kok et al., 2012).
To attend to these high rates of mental distress, the U.S. Veterans Health Administration (VA) has invested in ensuring the ready availability of clinicians trained in a range of first-line proven PTSD therapies, known as evidence-based therapies (EBT), for U.S. military veterans (Veterans Health Administration, 2023). Several therapies that are supported by strong randomized controlled trials are widely available and have a significant impact on symptoms. Indeed, VA has mandated that all veterans have access to one of the two most well studied EBTs – Prolonged Exposure (PE) or Cognitive Processing Therapy (CPT). In the largest head to head comparison of PE and CPT about two thirds of veterans receiving either therapy had a significant positive treatment response. (Schnurr, 2022). In response to this mandate, over 6,400 VA clinicians have been trained in the delivery of one or more EBTs (Karlin & Cross, 2014). There are also multiple medications, with sertraline (Zoloft) paroxetine (Paxil), and venlafaxine (Effexor) being the most strongly recommended first-line treatments that significantly reduce PTSD symptoms in randomized clinical trials, though indirect evidence suggests that they are inferior to the evidence-based psychotherapies (U. S. Department of Veterans Affairs, 2023).
Yet despite evidence of their effectiveness, many veterans with PTSD do not receive these therapies. First, many veterans with PTSD or associated clinical profiles are not recognized, particularly if they do not receive care from the VA, where PTSD screening is a routine intake procedure. Once recognized, many veterans do not receive (Hoge et al., 2014) or do not follow up on referrals for mental health care (Spoont et al., 2010). Finally, many veterans who initiate one of these EBT do not complete therapy – one review of the results in 20 studies estimated the dropout rate at 36% but noted that rates were higher, approximately 43%, in routine clinical care as opposed to clinical trials (Goetter et al., 2015).
Recognizing the high percentage of veterans who did not engage with these highly effective treatments, VA launched large-scale national initiatives beginning in the mid-2000s to increase use of EBTs, including PE and CPT as well as pharmacotherapy. In addition to extensive clinician training programs, the VA developed patient-facing educational materials, websites, and outreach programs describing PTSD symptoms, treatment options, and how these therapies work (U.S. Department of Veterans Affairs, National Center for PTSD, n.d.). These efforts were complemented by psychoeducational components embedded within post-deployment health screenings, reintegration programming, and specialty PTSD clinics, all intended to increase veterans’ awareness that effective treatments exist and are accessible through VA (National Academies of Sciences, Engineering, and Medicine, 2014). Studies show that national awareness initiatives and digital education tools—including web resources, mobile applications such as PTSD Coach, and nonprofit outreach programs—have improved mental health literacy, reduced stigma, and increased favorable attitudes toward treatment (Kuhn et al., 2017; Wounded Warrior Project, n.d.).
These strategies have substantially impacted the use of EBT within the VA system, but have fallen short of goals (Spoont et al., 2015). When veterans engage in these therapies, most experience clinically meaningful reductions in PTSD symptoms, and a substantial proportion of veterans who complete treatment no longer meet diagnostic criteria for PTSD (Resick et al., 2017). At the same time, studies consistently show that less than half of veterans who need mental health care receive it, and among those who do receive care, only a minority receive evidence-based psychotherapies (Seal et al., 2009). Of those who do, dropout rates for CPT and PE are high, ranging from 35–63% (Imel et al., 2013).
As a result, recent programmatic and research efforts have increasingly emphasized approaches that extend beyond general information dissemination, including peer-facilitated education, motivational engagement strategies, and navigation support models designed to help veterans translate knowledge about PTSD treatments into initiating care-seeking and sustained participation in evidence-based care (Kehle-Forbes et al., 2016; Kuhn et al., 2017).
There is a large body of research suggesting peer influence strongly impacts the behaviors and opinions of veterans (Mercier et al., 2023). Tailored educational materials that are relatable are essential to build trust and credibility needed to help veterans understand symptoms and engage in treatment (U.S. Department of Veterans Affairs, Veterans Experience Office, 2024). Collaborative design (co-design) is a component of community based participatory research (CBPR) and through prioritizing shared decision making and equitable collaboration, is an effective method to address the need for tailored communications and education (Franco et al., 2023; Hooyer et al., 2020).
CBPR aims to involve community members in all levels of research to develop relevant interventions that respond to community needs. Interventions that are co-designed by veteran peers are particularly effective in engaging veterans and empowering them to make decisions (Barker et al., 2023), to improve patient engagement and reduce stigma (Harvey et al., 2023), and to develop relevant health service interventions (LaMonica et al., 2019). Co-design, with its focus on creating culturally relevant materials with peers of the people for whom the materials are intended, is well-suited for a peer-led intervention aimed at improving PTSD treatment uptake among veterans.
The goal of this paper is to examine a community-engaged co-design effort in which veteran peer mentors and academic partners collaborated to develop educational materials intended to increase awareness and acceptance of evidence-based treatments for PTSD. In doing so, we describe the collaborative design process through which these materials were developed and refined, as well as the specific outreach products that emerged from this work. The paper is organized to differentiate the co-design activities from the resulting materials, with the methods section emphasizing the collaborative development process and the results section outlining the educational tools that were produced and iteratively modified over time. Particular attention is given to the role of concise, veteran peer-informed outreach materials—including the use of 4×6 informational “conversation” cards—as examples of how veteran perspectives were translated into accessible educational resources for broader community dissemination.
Materials and Methods
The project was submitted to the primary investigators’ institutional review board and was determined to be a quality improvement project.
The Reclaiming Your Path Program
We and partner veteran service organizations (the American Legion Department of Wisconsin and the Wisconsin State Council of the Vietnam Veterans of America) were funded by the Patient Centered Outcomes Research Institute (PCORI) to facilitate dissemination of the evidence supporting PTSD therapies to affected veterans. We used a veteran co-design approach to tailor existing summaries of the evidence to enhance veterans’ capacity to talk with their peers about the benefits of EBTs for PTSD. The veteran co-designers named the program “Reclaiming Your Path” and designed its logo, website, and educational content to support outreach activities.
Theoretical Framework
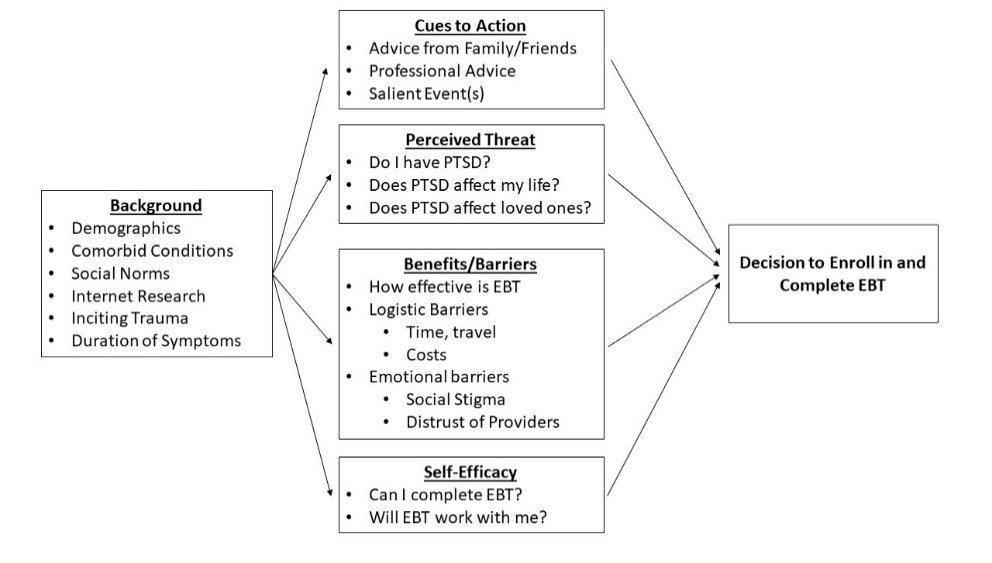
We used the Health Belief Model (HBM) (Becker & Maiman, 1975) as a theoretical framework to organize the reasons why veterans may not seek EBTs and to identify entry points for peer influence. The HBM was originally developed to better understand the adoption of health promoting behaviors, including the use of preventive services. The model has been adapted to explain the decision to use treatments for a variety of conditions, including PTSD (see Figure 1) and other mental health conditions (Cushing et al., 2018; Dillon et al., 2020). We worked with veteran volunteers with personal or peer experience with PTSD to develop ideas for promoting EBTs (e.g., enrolling and completing treatment) through educational materials and to determine the most appropriate ways to translate EBT for the veteran community (e.g., the military metaphors, language, imagery, and depth of information that would be most effective).
_by_veterans_wit.jpeg)
Recruitment
A critical aim of this project was to tailor existing messages around EBTs for PTSD in a way that better aligned with veterans’ needs and communication styles. This involved recruitment of veterans in a Midwestern city who had positive experiences with EBTs for PTSD. We recruited through clinicians who referred veteran patients, the project team’s previous programs, and our community partners.
Since PTSD affects both combat and non-combat veterans, we were deliberate in recruiting veterans from different backgrounds. This included different branches of the military, eras, gender, military specialties, PTSD symptoms, and treatment experiences.
We successfully recruited a diverse group of ten veteran partners. The group included representatives from the Army, Navy, Marines, and Army Reserves: two identified as women, three as African American, and two as Hispanic. They represented service periods ranging from the Vietnam War to the Global War on Terror. As trusted sources in the community, most of the veteran partners had worked or were currently working in veteran service organizations or as peer specialists. These veterans were offered compensation of $50/hour for their expertise, although several declined compensation since they thought it fit with their primary job or might affect their disability compensation.
This veteran partner group provided sustained participation in the creative development of outreach materials. A team of civilian community engaged researchers facilitated the co-design sessions: A medical anthropologist experienced in CBPR and collaborative design, a VA clinical psychologist specializing in PTSD interventions and peer support, a VA primary care physician with expertise in PTSD medications and peer support, and a project coordinator experienced in community engagement with veterans. The medical anthropologist worked closely with a graphic designer well versed in military culture to assist with product development iteratively with the veteran partner team.
Approach
The team met monthly for two years, for 90-minute sessions over lunch at an American Legion Post. The first year focused on co-designing outreach materials and educating veteran partners (peer mentors) on EBTs. We focused specifically on how veteran peer mentors might talk about these therapies with other veterans. Initial meetings had an MD present information about pharmaceutical EBTs for PTSD, and the behavioral science group present information about the EBTs for talk therapy. Next, PCORI - generated informational flyers for EBTs were shown to the veterans in small groups, and veterans were prompted to brainstorm ways that these flyers could be made more veteran specific and engaging for the veteran population. During these discussions, veteran partners were asked to come up with a veteran facing name for the project that encapsulated their perspectives rather than the academic team who wrote the grant. As we progressed through the co-design process, the veteran partners also suggested areas beyond the original scope of the project that they viewed as critical to advancing the underlying agenda of improving veteran uptake of mental health care.
In this sense, the meetings functioned as a form of participatory design laboratory in which professional expertise (medicine, psychology, anthropology, and graphic design) and veteran peer expertise were deliberately braided together to produce culturally resonant materials and messaging. This orientation aligns with traditions of CBPR that emphasize shared authority, in this case for problem framing, prototyping, content, and language, between designers and community stakeholders (Chen et al., 2020; Sanders & Stappers, 2008; Spinuzzi, 2005).
Consistent with these traditions, the collaborative work unfolded through repeated cycles of clarification, ideation, development, implementation, and iteration. Each stage involved structured opportunities for veteran peers to critique, reshape, and extend proposed materials, thereby shifting the design process from expert-driven dissemination toward community-informed knowledge translation. Importantly, the process also expanded beyond the initial scope of the grant, as peer mentors surfaced additional priorities they viewed as necessary to meaningfully advance outreach around PTSD treatment within veteran communities. Such emergent agenda-setting is widely recognized in participatory design scholarship as a marker of authentic collaboration, reflecting the transition from consultation to co-production of knowledge and intervention strategies (Sanders & Stappers, 2008). Through this iterative engagement, outreach materials were progressively refined to reflect veteran language, imagery, narrative practices, and modes of interpersonal trust-building, illustrating how collaborative design processes can transform the communication of clinical evidence into forms that are culturally legible and practically usable within community networks.
To structure reporting of this process, we adapted existing creative process approaches (Han, 2022; O’Donoghue, 2022) into five key steps that we use to summarize the dialogue that occurred: Clarify, ideate, develop, implement, and iterate. We then applied these steps in multiple cycles in the development of the informational conversation cards that veterans used as entry points to discuss EBTs.
Step 1: Clarify
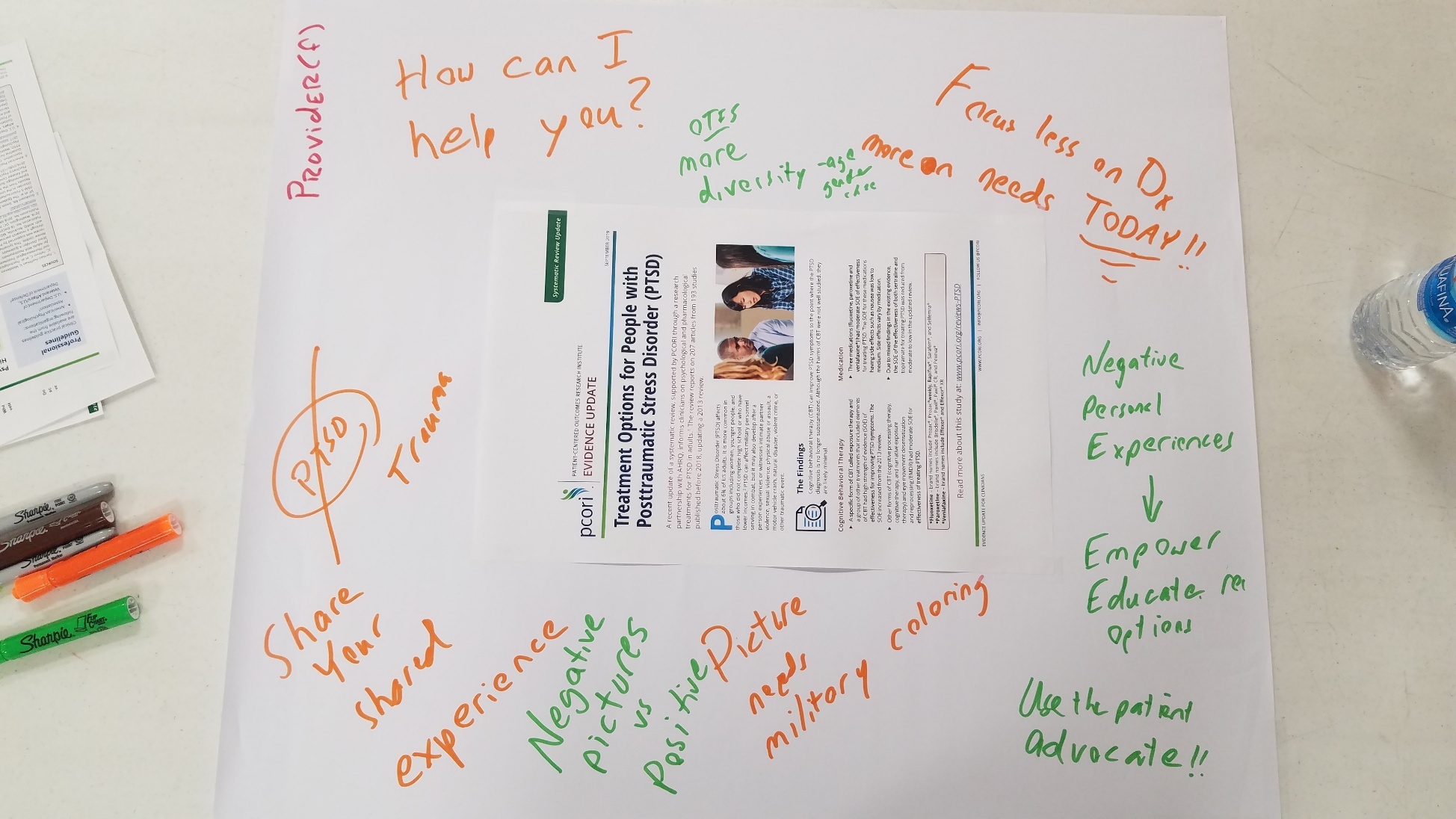
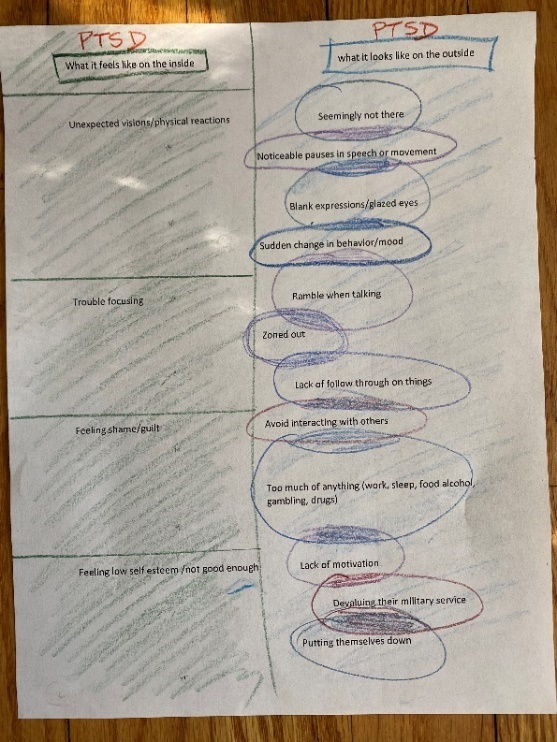
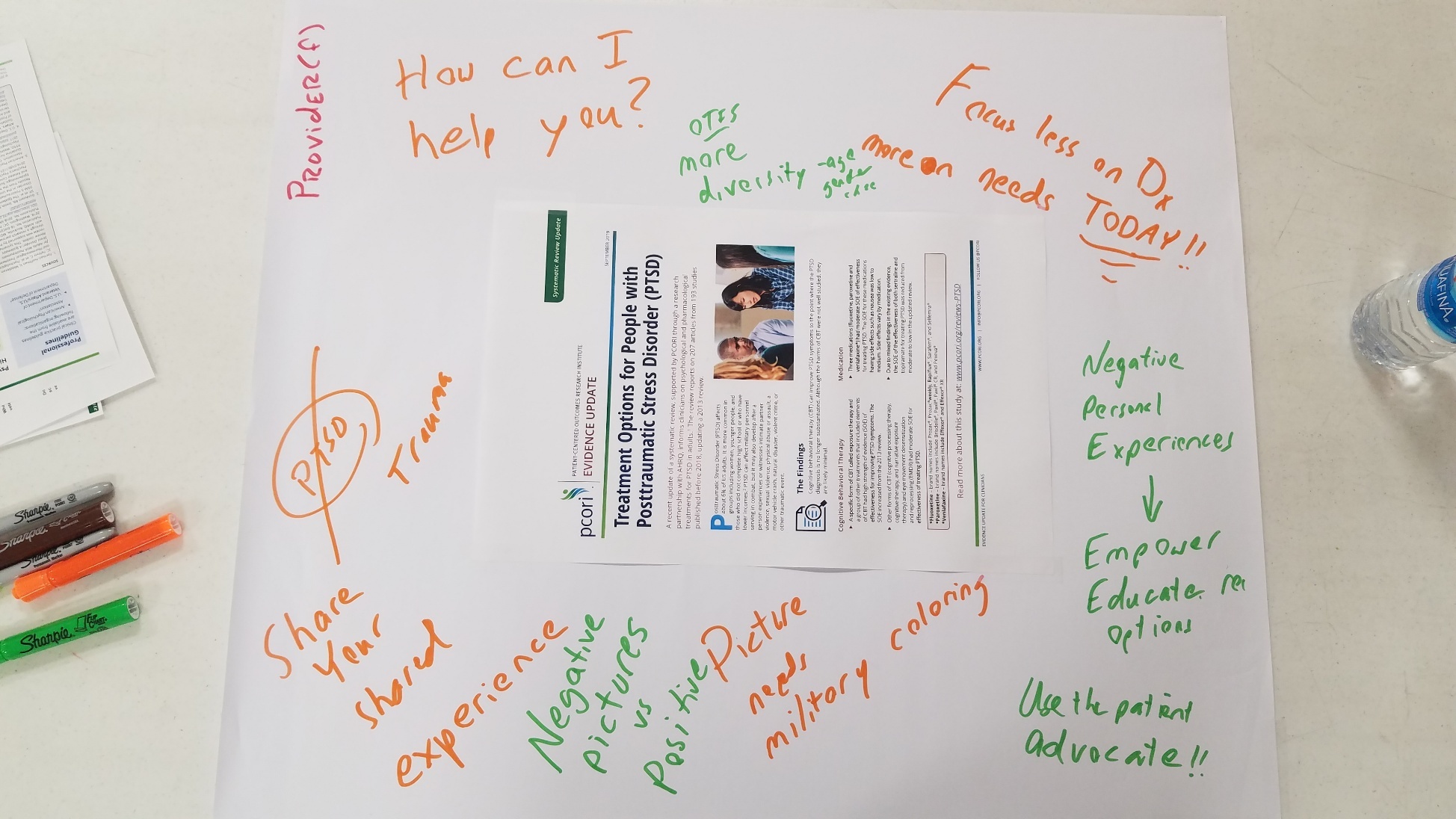
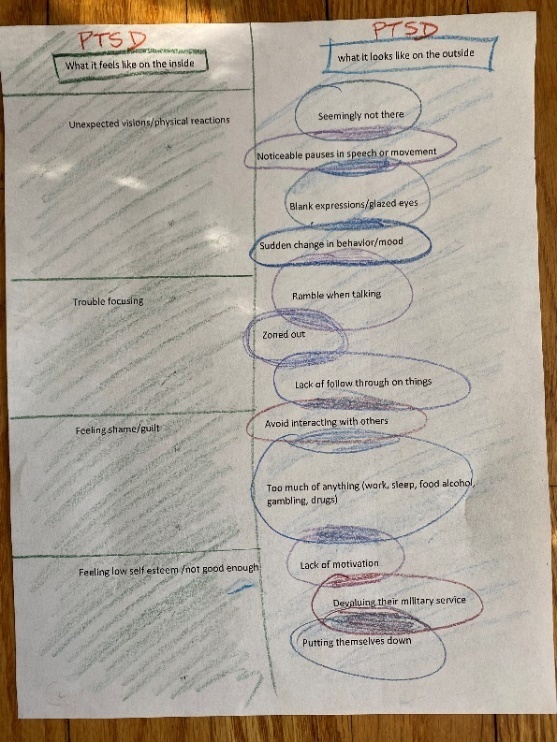
In this step the project team clarified the problem and how it might be solved. While recruiting veteran partners for the project, we simultaneously reviewed what is currently available online about PTSD and EBT, with a particular focus on public health information about PTSD provided by PCORI itself for patients and providers. We also hired a graphic designer with experience designing for a veteran audience. In our team meetings we asked: Do these resonate? What works? What doesn’t work? In small groups, our veteran peers made notes on these items (see Figure 2). The academic team collected these notes to come up with ideas for the veteran partners to respond to in the next meeting (Step 2).
Step 2: Ideate
Using a combination of brief presentations and table work, existing consumer education about EBTs for PTSD were provided in printed form for group discussion and critique (see Table 1). In this step we came up with ideas for improved materials that our graphic designer could prototype. We started considering imagery and language that might be effective, renaming the project (our grant title was very long) to state the intention of the group, exploring mediums (e.g., cards and website), and branding such as logo design and color palette.
Step 3: Develop
In this step the medical anthropologist worked with the graphic designer, translating ideas into a culturally tailored communication. Early on we shared design content with veteran partners before meetings, requesting feedback to start revisions before the next group meeting. However, we found it more effective to allocate time in the meeting for veterans to respond individually by making notes on copies of the mock-up first and then discussing their edits as a group.
The anthropologist made notes of all feedback during these meetings, collated drawings and detailed notes from the veteran partners and academic team and then met with the graphic designer to develop a first draft of a mock-up.
Our graphic designer, having worked with the project team on three previous veteran co-design projects, was in tune with the veteran experience of PTSD (e.g., symptoms and how PTSD plays out in daily life) as well as marketing science. For example, in designing one of the symptom description cards, someone on the project team requested darker camouflage and our designer responded with:
I think we should stay within branding. On that thought, to make these [cards] camo or darker they might get lost when a veteran gets them home. The bright colors help with identifying something different on their table. I have included a set with camo [for review].
Typically, co-designed elements (e.g., informational cards) took four cycles of refinement; the first and second cycle would come from the academic team and veteran partners, third cycle from the veteran partners for final review, and the final cycle from our project coordinator who would proofread everything.
Step 4: Implement
In this phase the veteran partners used the informational conversation cards we co-designed in their community outreach. Veteran partners relayed feedback from these experiences and shared strategies for using the cards, along with responses from the veterans they were in contact with. This essentially operated as a community of practice among our veteran partners, discussing “what worked” in specific circumstances and how they utilized the educational materials.
Step 5: Iterate
Once the veteran partners were doing outreach, we had multiple opportunities to iterate and tailor these communications. While the conversation cards were typically finalized and approved in Step 3 to save on printing costs, we did revise the PTSD Medications card after implementation to reduce the amount of information and convey more inviting (“not scary”) and simple language.
Results
The project resulted in veteran-led designs of multiple outreach materials. Our results will focus on: Branding that was veteran-focused and carried “street credibility”, and a set of PTSD and EBT educational pieces, that we describe as conversation cards. The project name and iconography (branding) necessarily preceded and influenced the development of these informational conversation cards.
New Project Title, Ethos, and Design Elements
The veteran partners co-designed the identity of the project by retitling it as “Reclaiming your Path | Life Nav” (RYP) which included these elements of brand design: Mission, purpose, color palette, imagery, logo, tagline, and call to action. The focus of the project, as conveyed on the website is to “make sense of the options that are out there so you can make informed decisions” because after military life “finding our way back can be frustrating without navigation skills and back up.” Veteran partners emphasized the importance of the program using language and visuals that tap into prior military training in order to both capture attention, and to put the goals of the training into an existing cognitive framework for the veteran.
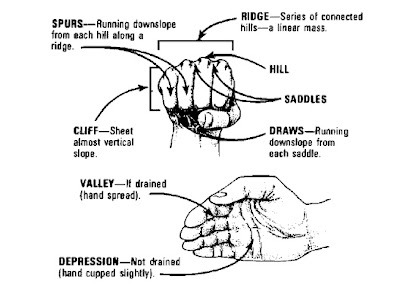
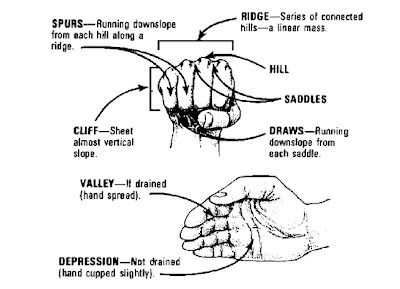
Through discussion, one consistent military training component that occurs across all branches of service was identified as land navigation. One of the veterans brought a US Army Field Manual (FM) and Soldier’s Manual of Common Tasks to make this point (Department of the Army, 1990). The veteran shared the skill sheet for “Identify Terrain Features on a Map” (p. 61 of the above Soldiers Manual) with the academic partners. Famously in military circles, this skill involves using one’s fist to describe major terrain features (see Figure 3), and it has become ubiquitous across branches. Here, the importance of embodied cognition and mnemonics in teaching survival skills for low resource environments or being able to recall these elements while under fire came to the fore with the notion that veterans in the midst of mental health difficulty similarly need to key into metaphors that activate prior military learning in order to instil a sense of hope and potential for mastery of the situation (Flood & Keegan, 2022).
Next, discussion around orienteering and visual metaphors for getting off track with mental health during civilian reintegration were explored. Training mnemonics like OAKOC (Observe, Avenues of Approach, Key Terrain, Obstacles, Cover and Concealment) and SPLASH (Start, Plot, Landmarks, Azimuth, Steps, Handrails) came into the discussion. Veteran peer mentors drew additional parallels between SPLASH in particular and the process of civilian reintegration, noting the importance of identifying a final objective (reintegration), setting map orientation (perhaps broadly seen as a recognition that the veteran has become disoriented from civilian life), shooting an azimuth to get a bearing (deciding to work toward reintegration and selecting a direction toward the objective), and using terrain elements in between current location and the objective to create checkpoints where bearings can be retaken (a recognition that the path may to reintegration may not be as straight as the original plan, requiring episodic recalibration). The idea of navigating to a ridge, or higher ground, was broadly equated with success in reintegration into civilian life.
Using this feedback, several notional images were created by the graphic designer. These were presented to the veterans in an online survey to obtain brief individual feedback. These images included a person with the sun in the background (hope/warmth/confidence) water (life/healing/naval manoeuvres), compass (direction/guidance/finding one’s way), falcon (intelligence/precision/powerful); along with stock photo montages of groups of military personnel (fellowship/support/trust), veterans clearly depressed or receiving mental health support (disengaged/needing help/seeking hope) and non-military photos of an individual in nature at sunrise with a horizon line clearly visible (hope/gratitude).
Responses to the images suggest that the process may have been a bit vague for the veterans, but the process helped crystalize the group level discussion around using more positive, less military focused imagery and project naming strategies, straddling the goals of ensuring the program could be easily recognizable as veteran focused by former military service members, but also deemphasizing military iconography in order to place emphasis on positive civilian reintegration and transition toward a more integrated post-service identity.
The veteran partners chose the symbol of a lensatic compass as the core iconography for the project since navigation is a core military discipline and recognizable by all branches. The compass motif was entirely driven by veteran input, both because of the self-reliance that it implied, and because it was something that you had to learn to use. As a metaphor for treatment and trauma healing the entire group agreed on this, even though not all branches used the lensatic compass.
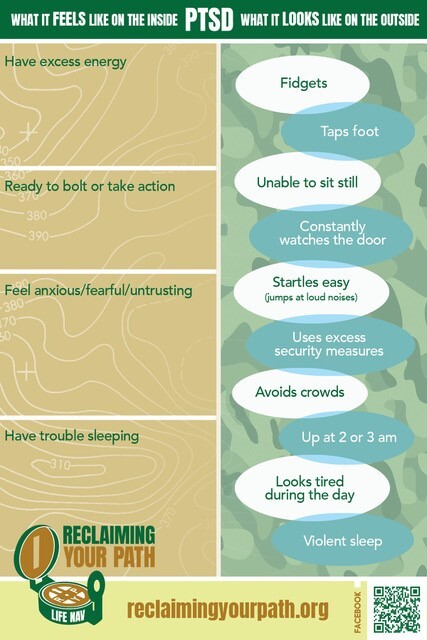
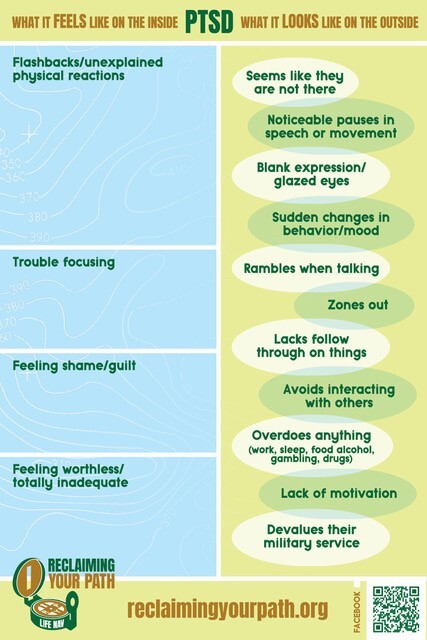
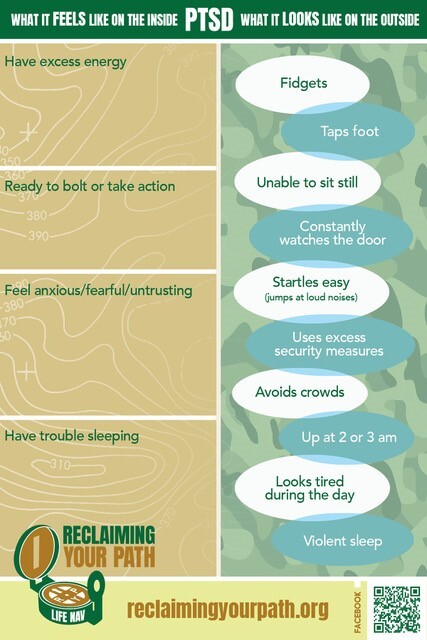
Contour lines representing sea elevation were added as inclusive design elements (since the Navy and Coast Guard emphasize ocean navigation) based on feedback from veterans in the group who had served in the US Navy. They suggested that this modification, merging land and sea mapping techniques would be simple solution. Notably, for most of the designs traditional military camouflage was avoided, and brighter colors were chosen to “uplift,” help represent a “transition to civilian life,” and differentiate RYP from more corporate entities. The only card where camouflage was reintroduced was the PTSD Signs and Symptoms card to link it specifically to military PTSD, in contrast to other forms (e.g., civilian, natural disasters).
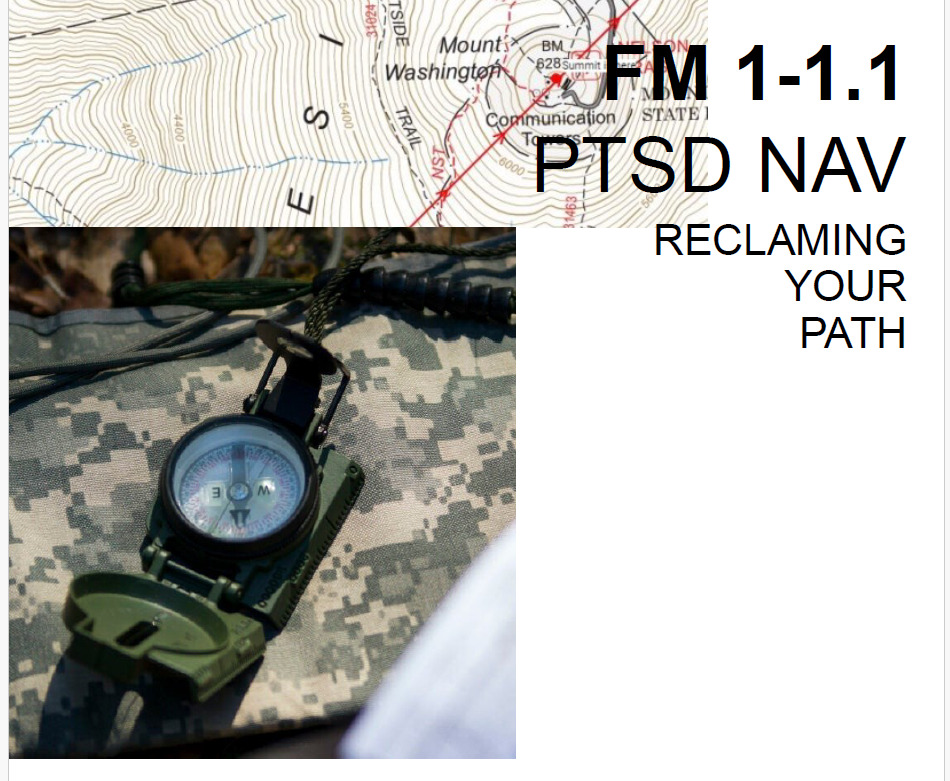
Naming alternatives for the project included Trauma to Triumph, PTSD NAV, Life NAV, and Reclaiming Your Path. A mock-up of a possible designs incorporating several of these elements was provided for discussion (see Figure 4). Veterans voted privately on these names using an online survey platform, Qualtrics, with Life NAV and Reclaiming Your Path being clearly preferred. Returning results of the individual responses to the naming survey and the mock-ups provided foundation for a final group discussion where the name Reclaiming Your Path was selected. The consensus process used to select the final name highlighted the ideas that Reclaiming Your Path avoided the military specific feel of the alternative name Life Nav, it suggested an action orientation, and it incorporated subtle elements of land navigation training that focus on checkpoints along a pre-planned path where reorientation may be required. Graphical themes approximating a design guide were developed based on these discussions including a stylized lensatic compass logo, color palette, and imagery that were later applied to the project’s outreach materials and 4x6 conversation cards requested by the veteran partners.
With the foundation of a project name and iconography that the veterans felt matched the mission of this work, we moved on to design consideration around the educational content. The co-designed supplementary educational components to support veteran peers in their outreach mission included: Four conversation cards and one advocacy card.
Early in the clarify stages the problematic components in current PTSD and treatment educational materials the project team reviewed (see Table 1) included: Too “corporate;” some are good but can’t be found easily; and some have a “VA style” that was felt to be less accessible (over emphasizing recovery or “selling” EBTs that some veterans may not be interested in). We also learned that less is more and too much detail could be off-putting and even threatening in its clinical approach, which could be read as inauthentic from a veteran standpoint. This was especially true for veterans who had mistrust in the medical system or government authorities based on their past experiences.
PTSD and EBT Conversation Cards
We collaboratively created 2-3-page summaries for four talk therapies and four medications to support veteran partners in their outreach. In developing these summaries, key information veteran partners wanted became clearer. For talk therapies, mechanism of action, duration of treatment, drop-out rate, evidence summary, what therapy might look like week-by-week, the need to complete homework, and requirement to discuss specifics of the trauma were viewed as key areas where lack of information might cause a veteran to not seek care.
For medications, side-effect considerations including weight gain, light-headedness, erectile or orgasmic dysfunction, arrythmias, sedation and insomnia; time to action; hypervigilance, and reexperiencing, while often improving sleep; and logistical considerations such as time to symptom improvement, best time of day to take the medication, impact of a missed dose, and ability of a primary care physician to prescribe were all identified as important informational elements to include.
In the ideate stages veteran partners frequently steered conversations from our academic priority of promoting EBT to recognizing PTSD (observable and felt signs and symptoms) and accessing care (e.g., the challenges some veterans faced visiting the VA or non-VA providers with limited awareness of the nuances of military PTSD). There was a major shift from our grant objective of disseminating messages regarding EBT use and its likely benefits, to the veteran partners’ objective to “just get them in the door” into any kind of care. Our veteran partners were more concerned with veterans “falling through the cracks” than getting treated with an EBT, and importantly, able to make informed decisions on their own with proper information.
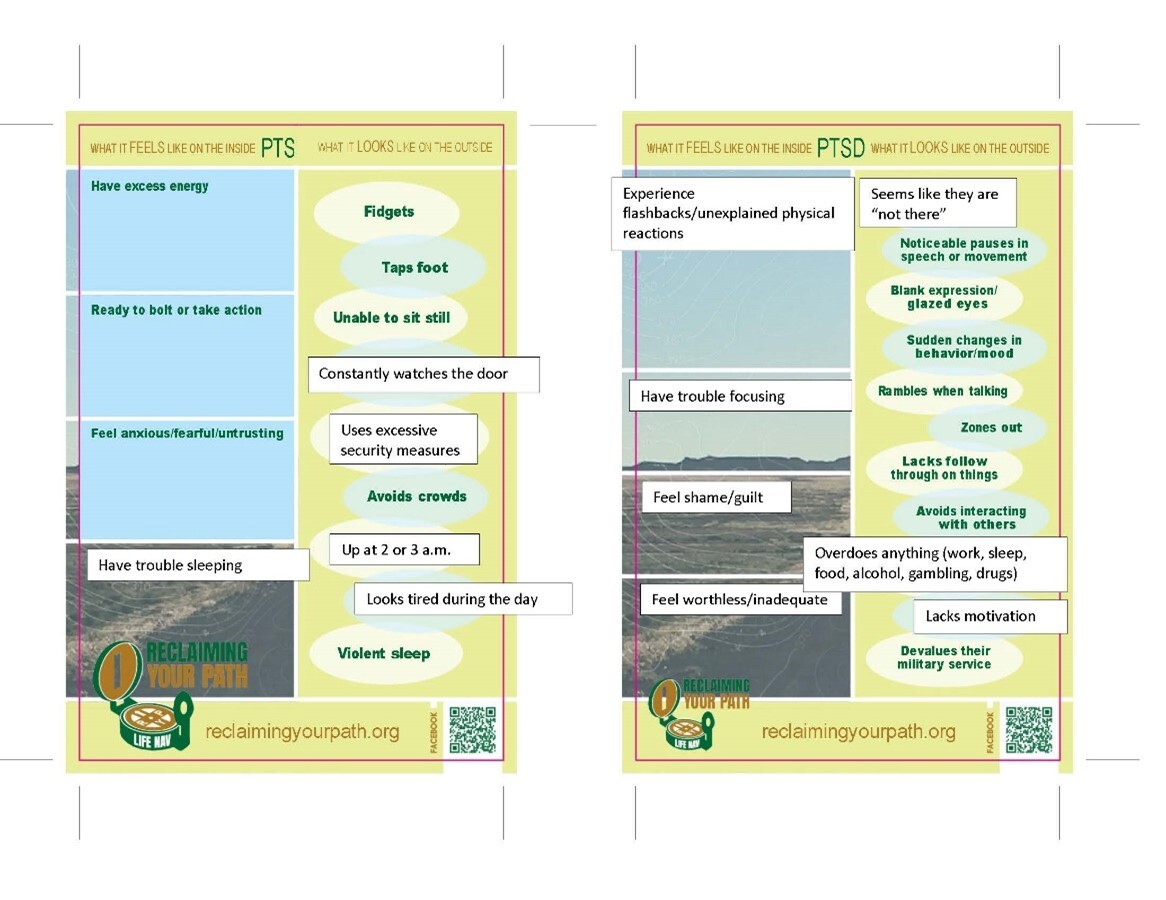
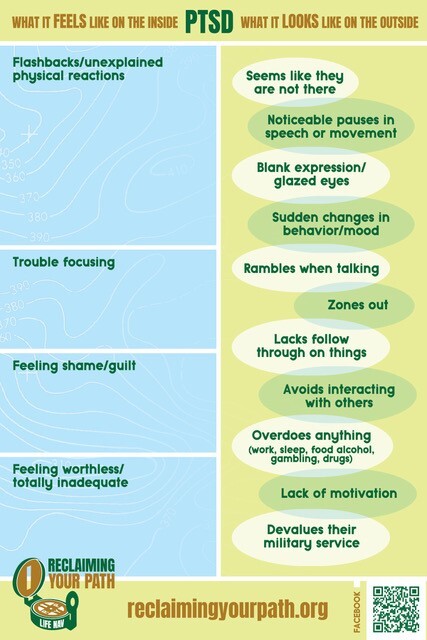
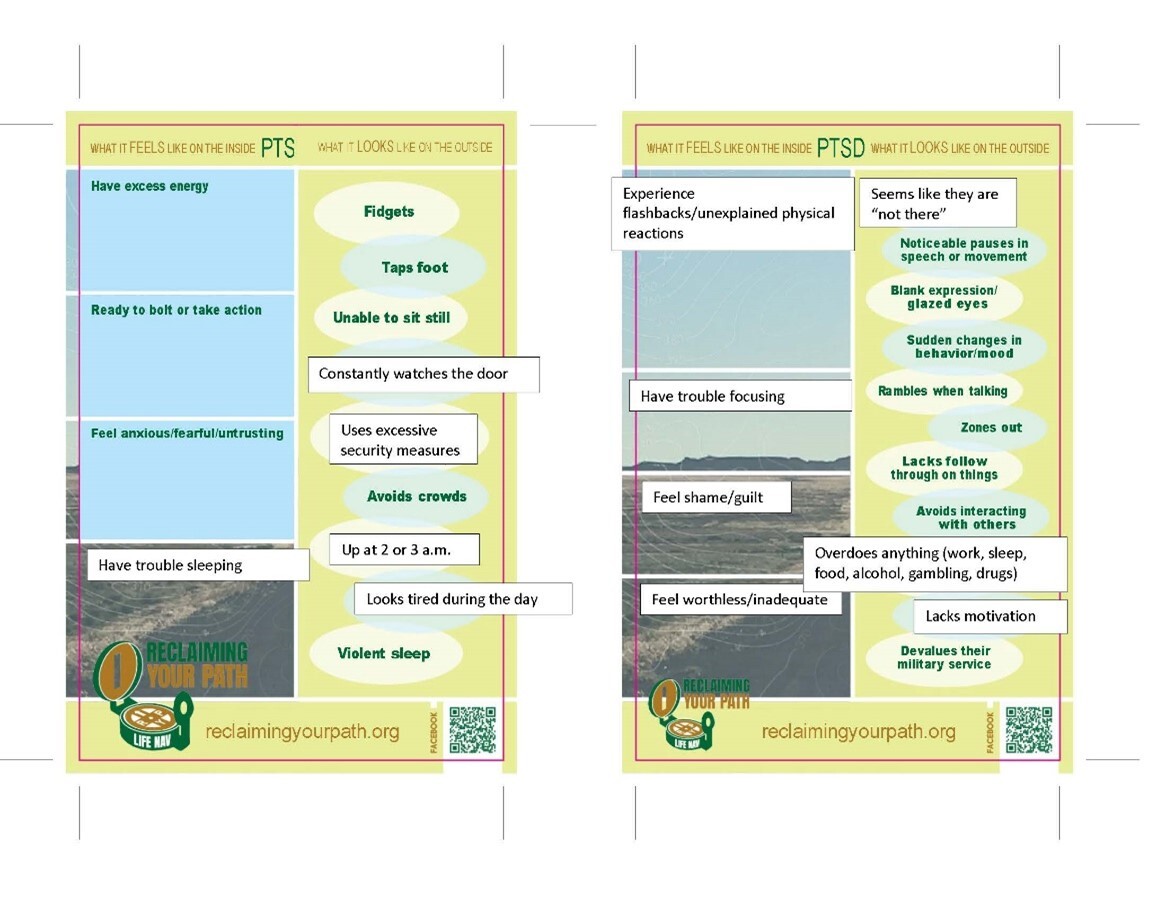
The develop stages revealed the need to provide easily accessible reference materials. The original 8.5x11 summaries were clunky. The move to 4x6 cards that could “fit in a back pocket” was inspired by military education that included small booklets that could fit easily in a uniform pocket or rucksack. The academic team was also reminded that veterans with PTSD and traumatic brain injury have memory and focus issues and may present with these symptoms in doing outreach. Veteran partners iterated time and again that the language be clear and succinct and essentialized to contend with these realities – for both the veteran peer giving the information and the receiving veterans (see Figure 5).
Below is an example of these iterations (see Figures 6-10). The 4x6 conversation cards operated as tailored forms of psychoeducation intended to replace “corporate” and “clinical” brochures typically found in civilian doctors’ offices or at VA facilities.


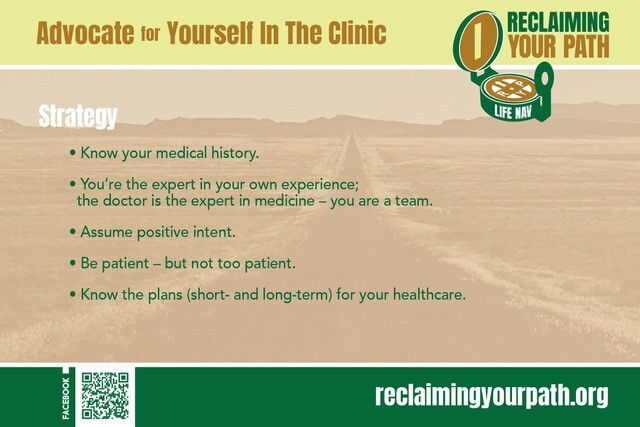
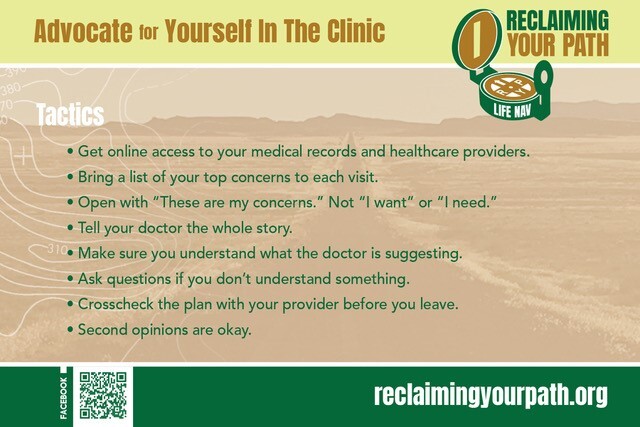
Self-Advocacy Cards
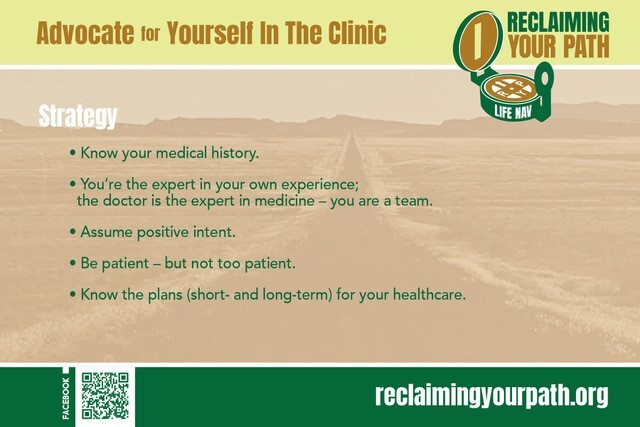
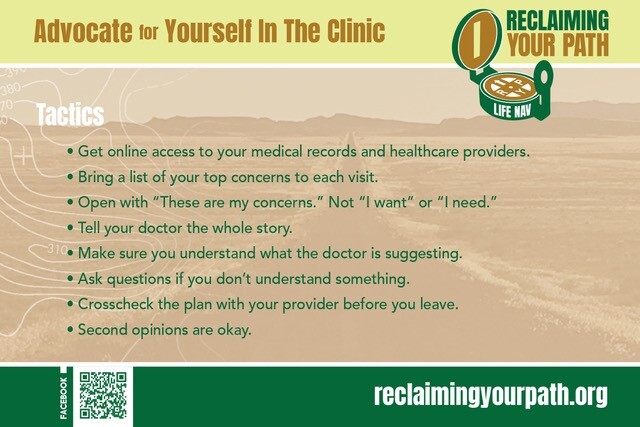
In the implement and iterate stage, the focus of veteran partners on getting veterans into any care versus engaging veterans in EBT treatment led to discussions on how to empower veterans to ask the right questions once they were “in the door.” This led to the development of a conversation card that doubled as a “leave behind” (giving veterans these cards as Field Guides for their clinical encounters). These cards focused on strategies and tactics for self-advocacy in the clinic (see Figures 11-12). This was not related to any of the project team’s original EBT grant objectives and emerged from the veteran partners’ concern that “it doesn’t matter” which therapy veterans start with; they just need to get started with something. The key items that veteran peers recommended for self-advocacy included: Know your medical history and how to access your medical record; avoid “telling the doctor what you want,” rather “explain concerns and make sure they are addressed” by the doctor “to your satisfaction;” follow up on concerns with your doctor via healthcare messaging platforms or phone calls; and be sure to ask about options.
RYP veteran partners successfully distributed these 4x6 conversation cards to individual veterans, VA primary care providers, and veterans’ organizations. We also made them available online and the website includes downloadable versions of the cards that can be printed at home or professionally. A full downloadable toolkit with all components was developed so others could replicate the process for different audiences, available at https://reclaimingyourpath.org/# under Resources.
Outreach ranged from formal tabling at veteran resource events including mental health conferences and job fairs, to social events like the annual air show or music in the park at the War Memorial Center. RYP veteran partners made short presentations at American Legion post meetings, where they shared information on the project and EBTs. Reported informal peer outreach including everyday social interactions, such as hanging out at baseball games, at the bar, or fishing outings.
One unanticipated outcome of the co-design process was the strong relationships that were forged, leading to a commitment to future RYP-related projects. Our veteran partners came to know each other and the academic team well, sharing intimate experiences around trauma. Having a VA clinical psychologist and VA physician on the team supported deep discussions around the practical issues of accessing VA care, and the multidisciplinary team seemed important to setting the stage for moments that brought the group closer together. The veteran partners who met with us monthly for two years had been engaged in helping fellow veterans with mental health conditions, whether professionally or personally. However, now they have developed relationships with each other and with academic members of the team that have facilitated continued collaboration on new grants, as well as continued outreach.
Relevance of results
We successfully developed culturally tailored messaging and materials that would allow veterans to transmit information about PTSD and evidence-based therapies to veterans as an alternative to the forms of broad public health education about EBTs for PTSD currently available. This was substantially more time consuming than expected because veterans strongly felt the need to increase the emphasis on recognition and referral of veterans with reintegration problems, (e.g., additional content including Signs and Symptoms, How to Ask about Symptoms, and the Advocacy in the Clinic cards) more so than specific guidance around the use of EBT. In other words, veteran peers felt it was more important to get veterans in need connected to care, no matter what that care looked like.
Our work, informed by the HBM, also identified that the barriers to entering treatment might be more important than resistance to using EBT in particular. The belief that veterans actively using therapies with less scientific support should be applauded for receiving a treatment, reflected the overriding interest of our veteran partners to not “push” EBT, but rather to respect what was working for that veteran.
These findings are highly relevant to both clinical providers and systems. They suggest that the veteran partners in Reclaiming Your Path demonstrated strong engagement around these mental health issues and expressed a desire to help ensure that their fellow veterans experiencing invisible wounds are identified and connected to care.
Because the academic team included clinicians, designers, and an anthropologist well versed in trauma interviewing, we were able to have a depth of conversation and vulnerability that led to a committed and supportive group. We had a clinical psychologist who could help move discussions beyond the exploratory to get to the core of the PTSD experiences, allowing for authentic representations that were more “on point” in the outreach materials.
In recruiting diverse veteran partners, along with our multidisciplinary academic team, we believe that RYP will continue to be able to expand contact with veterans from a wide range of eras. Most of our veteran partners have significant roles in one or more veteran-led, veteran-serving organizations, making this possible.
Challenges
We found that it was difficult to identify veterans who had personal experience with EBT and were able to stay with the project. Two veterans who stepped forward early in the project stopped attending after just a single meeting. Although they were familiar with at least one member of the academic team and with some of the other veteran partners they did not return for any follow-up meetings or respond to invitations to discuss any challenges they were facing. Since isolating behaviour is one characteristic symptom of PTSD, we worried that these two veterans may have been triggered by the project engagement. We did have intermittent contact with other people who knew them, and one or more members of the team did meet with each of them, unrelated to the project. We did not find any reason to believe that interacting with the project caused increased PTSD related difficulty. However, some veteran partners who stayed with the program noted that they were triggered by certain topics or when they described issues in their own reintegration or care seeking, underscoring that any teams working in CBPR should be alert for this possibility.
Of the ten veterans who committed to this co-design project only three had experiences with completing EBT with successful results. While a challenge, this may have contributed to the project’s focus on increasing the emphasis on recognition and referral of veterans with reintegration problems, rather than EBTs specifically.
We found that we could not drive as much traffic to our website as we thought would be possible. We could not solve this problem over the course of this relatively brief project. Since we have established relationships with an increasing number of veterans organizations and were awarded another grant to expand this work, we believe that we will be able to continue to gradually build membership, as we build content.
Conclusion
Post-traumatic stress disorder (PTSD) is a common and often debilitating condition for military veterans. Effective treatment exists but is under-utilized. The reasons for this are many and must be addressed from multiple angles. Barriers related to lack of awareness and/or scepticism about what works could be improved via education. It is well established that peer influence and support can impact the opinions and behaviours of veterans. We sought to leverage the skills and lived experiences of trained veteran peers to improve awareness and uptake of EBT for PTSD.
We recruited and trained a cadre of ten veterans in the basics of evidence-based psychotherapies and medications with proven benefit in PTSD symptom reduction. We simultaneously engaged these veterans in the co-design of educational assets related to these therapies, walking with them through the five steps of the creative process approach, i.e., clarify, ideate, develop, implement, and iterate. The process resulted in a suite of culturally tailored outreach materials used by the veteran peers and academic team in presentations, at community events, and in one-on-one conversations. They are also shared publicly via the internet and social media.
The final products reflected an emergent emphasis from the veteran peers on identifying the signs and symptoms of PTSD and connecting fellow veterans to any kind of mental health care, a divergence from the project’s stated goal of increasing awareness and use of evidence-based therapy. Viewed through the lens of the Health Belief Model, this change in emphasis suggests that lack of perceived threat and barriers to entering treatment might be more important than resistance to using EBT or concerns about EBT efficacy. In other words, if many veterans do not recognize that they have PTSD, or if they have been stymied by the bureaucracy of a health care system to the point of receiving little to no mental health care, educating them about optimal PTSD treatment puts the cart before the horse. Turning this around will require a closer examination of pre-treatment factors that contribute to inadequate use of evidence-based therapy for PTSD and continued collaboration with engaged veteran partners who are empowered by the co-design process and interested in developing interventions that best serve the needs of those who served.
Based on the learnings from the above effort, we recently obtained funding from the Advancing a Healthier Wisconsin endowment to expand the impact of this project by training a wellness navigator at American Legion posts and University of Wisconsin student veteran facing organizations in several counties across the state. Using the veteran-informed educational materials and outreach strategies developed in the initial project, navigators will be trained to recognize signs of PTSD, engage veterans in conversations about evidence-based treatments for PTSD, and connect them to appropriate clinical services. By embedding this role within existing community infrastructures, the Reclaiming Your Path Wisconsin program seeks to extend the reach of evidence-based mental health information and strengthen pathways to care for veterans who may not otherwise engage with formal treatment systems. We hope this approach provides a model for further integration of veterans’ voices into population level health education on PTSD, care access and acceptance, offering a scalable model for community-based dissemination of evidence-based mental health information among veteran populations.
Disclosure/declaration of interest statement
The authors report there are no competing interests to declare.