
Participatory research emphasizes community engagement throughout the research process, yet dissemination often remains a one-way transfer from researchers to communities. This positions community members as passive recipients rather than active interpreters of knowledge, reinforcing power imbalances and limiting opportunities for shared meaning-making (Israel et al., 1998; Wallerstein & Duran, 2006). Scholars critique this model for its limited capacity to support collaboration. Bowen & Graham (2013) argue that conventional “knowledge transfer” frames stakeholders as recipients of expert information while McDavitt et al. (2016) show how dialogic, reciprocal dissemination strengthens trust and accountability. In global health, similar critiques reflect how affected populations are often excluded from decisions about how findings are shared or translated into action (Jull et al., 2017; Mosavel et al., 2019).
Sickle cell disease (SCD) affects roughly 515,000 newborns each year, with more than 70 percent born in sub-Saharan Africa (GBD 2021 Sickle Cell Disease Collaborators, 2023). The condition causes recurrent pain crises, anemia, and life-threatening complications that contribute to high childhood morbidity and mortality (Kenney et al., 2024). In low resource settings, such as Kenya, families navigate both medical and psychosocial burdens, including emotional distress, financial strain, and limited access to comprehensive care (Ally & Balandya, 2023; Kuerten et al., 2020). Although psychosocial interventions for SCD have been developed and tested in high-income countries (Edwards & Edwards, 2010; Palermo et al., 2016; Sahler et al., 2002; Young et al., 2021), few have been adapted for African contexts where the need is greatest. Our work in Kenya aims to contribute to contextually grounded evidence to inform psychosocial care for families affected by SCD.
To advance this goal, we conducted 15 focus group discussions (FGDs) across three clinics in Western Kenya with adolescents living with SCD, their caregivers, and healthcare providers. Discussions explored the psychosocial experiences, challenges, and support needs. Using reflexive thematic analysis, a multidisciplinary team of Kenyan and U.S.-based researchers identified key patterns that informed the next phase of the project. We adopted a dissemination-as-design approach that treated dissemination as a starting point for intervention development rather than the final step. Grounded in participatory dissemination and Human-Centered Design (IDEO.org, 2015), this approach framed dissemination as a reflective and generative process, enabling communities to interpret and begin shaping potential solutions (Bazzano et al., 2017).This report describes participatory dissemination workshops with adolescents, caregivers, and community stakeholders in Kenya. We illustrate how dissemination transitioned into early collaborative design and highlighting methodological lessons for participatory research and global health practice. The workshops aimed to (1) return findings in an accessible and dialogic format, (2) Support shared interpretation and priority setting, and (3) use discussions as an entry point for co-creating psychosocial intervention ideas.
The Participatory Dissemination Process
Context and Partnerships
This project was conducted in western Kenya in partnership with Moi Teaching and Referral Hospital (Eldoret), Webuye County Hospital, and Homabay County Hospital. These facilities serve both urban and rural populations, providing care within resource-constrained contexts. The study was embedded in the Academic Model Providing Access to Healthcare (AMPATH) consortium, which offered trusted relationships and research infrastructure,
Focus Group Methods and Analytic Process
In brief, fifteen focus group discussions were conducted between July and August 2024 across the three sites. Participants included 54 adolescents and young adults with sickle cell disease across developmental stages ages 10 to 14, 15 to 17, and 18 to 25, as well as 18 caregivers and 18 healthcare providers. All discussions were facilitated bilingually in English and Kiswahili. Detailed sampling, recruitment, and analytic procedures are described in a prior manuscript (Ochieng et al., 2026).
Analysis followed a reflexive thematic approach using a hybrid deductive and inductive strategy (Braun & Clarke, 2006; Fereday & Muir-Cochrane, 2006). An initial codebook was developed from the FGD guide, with additional inductive codes generated through iterative transcript review. Seven researchers from Kenya and the United States participated in coding, including team members with lived experience of sickle cell disease, strengthening contextual interpretation. All transcripts were coded in NVivo Version 14.
To promote analytic consistency, five anchor transcripts representing each participant group were coded by one team member and independently reviewed by a second. Discrepancies were resolved by the senior author. The remaining transcripts were coded by designated team members and reviewed by at least one additional coder, with disagreements resolved through consensus discussion. Four cross-cutting themes were identified that informed the workshops: emotional distress and coping; family and peer support; barriers to healthcare access; and stigma and identity.
Participants
48 stakeholders participated across the three sites (Eldoret n=19, Homabay n=14, Webuye n=15) including 9 adolescents and young adults with SCD aged 16 to 28 years, including two minors who participated with written parental or guardian consent and personal assent in accordance with institutional review board approval. Additional participants included 11 caregivers, and 19 providers (nurses, clinical officers, physicians, and social workers). Workshops also involved 3 teachers, 2 school administrators, 1 faith leader, 2 national SCD advocates, and 1 village elder. This multi-sector representation reflected the socio-ecological environments that influence psychosocial wellbeing among adolescents with SCD. Detailed participant characteristics are presented in Table 1. Workshop participants were recruited using purposive sampling. A subset of prior focus group participants was invited to ensure continuity of engagement; alongside additional stakeholders identified in collaboration with clinical and community partners at each site.
Workshop Overview
Workshops were held in June 2025 and followed a two-day workshop at each site lasting approximately four to five hours per day. Day 1 focused on returning FGD findings and supporting participants interpretation. Day 2 translated shared insights into early-stage design concepts for psychosocial support interventions.
The overall sequence of activities is summarized in Figure 1, which outlines the two-day progression from findings return to reflection, empathy building, and early co-design.

Workshop Part 1: Findings to Interpretation
Presentation of Findings
Facilitators presented four themes derived from thematic analysis of the FGDs: emotional distress and coping, family and peer support, barriers to healthcare access, and stigma and identity. These FGD-derived themes were identified by the research team to provide the initial framing for workshop dialogue. Direct quotations were incorporated to allow participants to see their experiences reflected in the findings. Slides and printed handouts used large fonts, and facilitators alternated between English and Kiswahili to ensure accessibility. After each theme was presented, facilitators paused to invite reactions. For example, caregivers expanded on family routines and caregiving fatigue, while adolescents spoke about the social costs of stigma and absenteeism in schools.
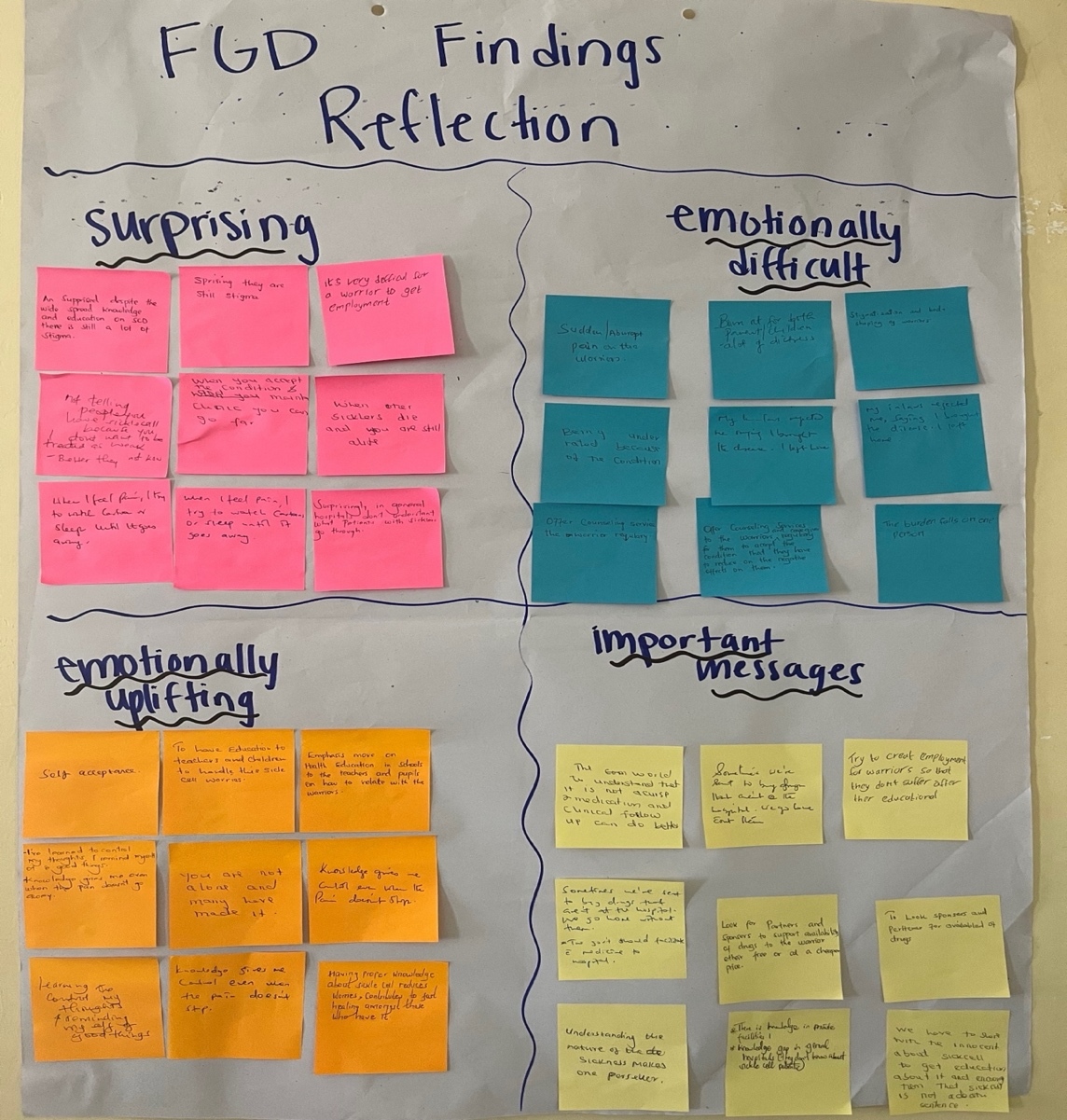
Next, participants completed a reflection activity. Each participant received 4 color-coded sticky notes and was asked to brainstorm with a partner about the findings. Red notes captured “what stood out for you.” Blue represented “anything that felt hopeful or emotionally uplifting.” Yellow reflected “what felt hard or emotionally difficult.” Green captured “important messages that should guide the creation of effective psychosocial interventions.” After writing reflections, participants posted their notes in the corresponding quadrants on a flip chart. Facilitators reconvened the group and invited volunteers to share insights from their discussion or from others’ reflections.
This activity highlighted nuances that were less prominent in the original analysis. For example, while earlier findings emphasized stigma and healthcare barriers, participants elevated sibling burden and school-based challenges as urgent priorities. The exercise demonstrated the analytic value of participatory interpretation and how community members naturally extend researcher-generated themes.

Challenge and Support Mapping
Participants next engaged in a Challenge and Support Mapping exercise designed to expand the problem frame beyond the original thematic structure. Individually, participants wrote challenges they had experienced or observed on pink sticky notes, one per note. For each challenge, they identified either existing or potential support on a yellow note. Existing supports were marked with a star to distinguish them from new ideas.
Facilitators organized the notes into four columns on a large wall chart corresponding to the four themes and invited volunteers to cluster similar challenges and support within each column. All outputs were photographed and documented in written synthesis notes. These materials were reviewed during end-of-day team debriefs and directly informed Day 2 ideation prompts. Priorities that emerged through this activity, including sibling burden and specific school-level barriers, were intentionally incorporated into subsequent design exercises.
Empathy Mapping
The second half of day 1 of the workshop marked a transition into the first stage of Human-Centered Design: Empathy. Empathy mapping is a structured method that supports perspective-taking by prompting participants to consider the needs, constraints, and motivations shaping another person’s experience. Each group received a “persona card” introducing a composite character grounded in the FGD findings and the team’s contextual and clinical knowledge of psychosocial challenges. They provided pre-structured starting points developed by the research team, grounded in FGD findings and contextual and clinical knowledge of psychosocial challenges. Personas represented typical individuals in the SCD care ecosystem, including adolescents, caregivers, and healthcare providers.
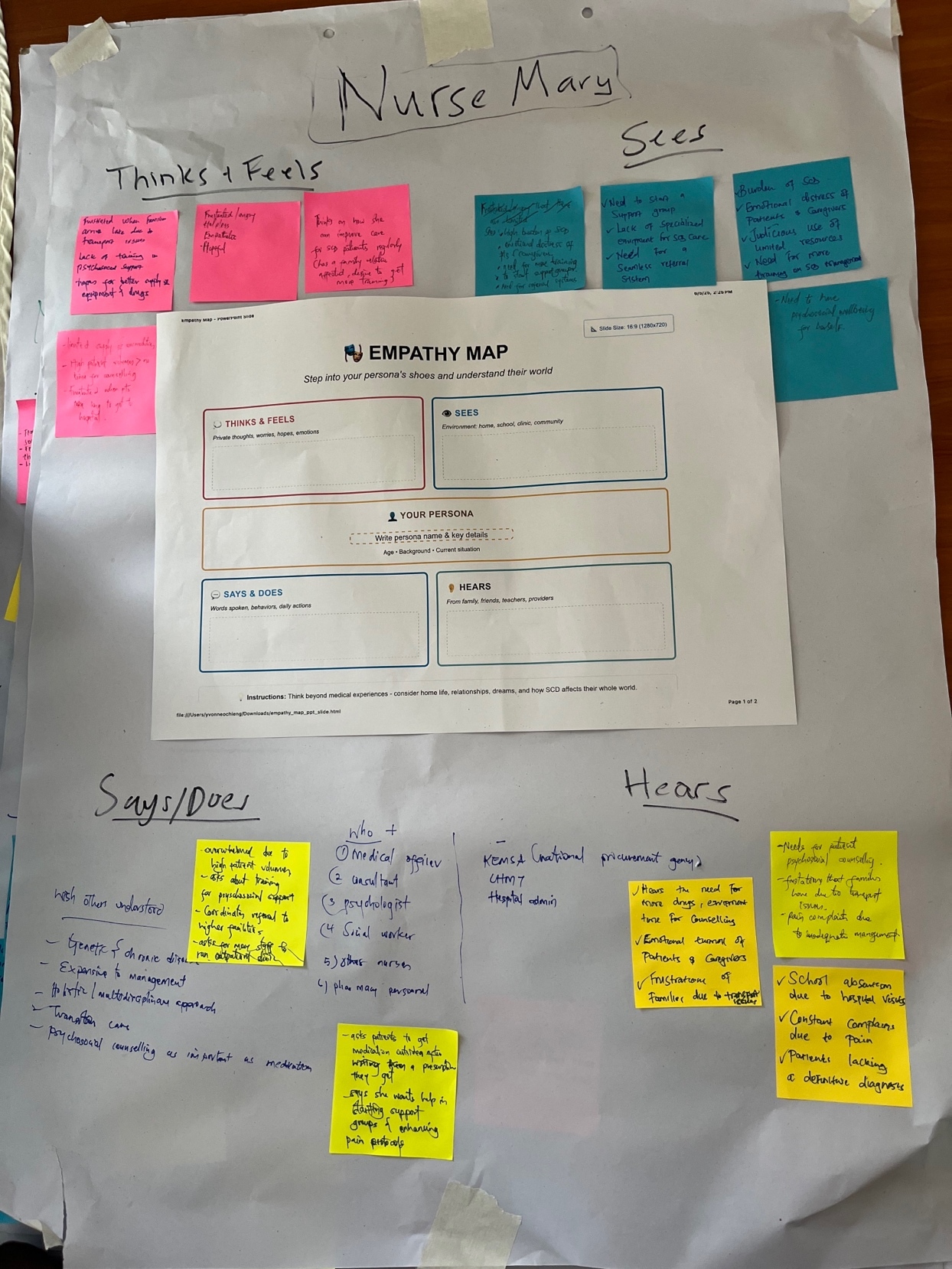
We adapted a large format “empathy map” template from the IDEO toolkit (IDEO.org, 2015), which included four quadrants (“Thinks and Feels,” “Says and Does,” “Sees,” and “Hears”) with a center space for the persona’s name, age, background, and contextual details. Working in groups of four, participants reviewed their persona card and discussed what they believed this individual might “think”, “feel”, “see”, “hear”, and “do” in daily life across home, school, clinic, and community contexts. Each small group included a facilitator who remained with the group throughout the activity to guide discussion, clarify of each quadrant, and prompt deeper discussion when needed.
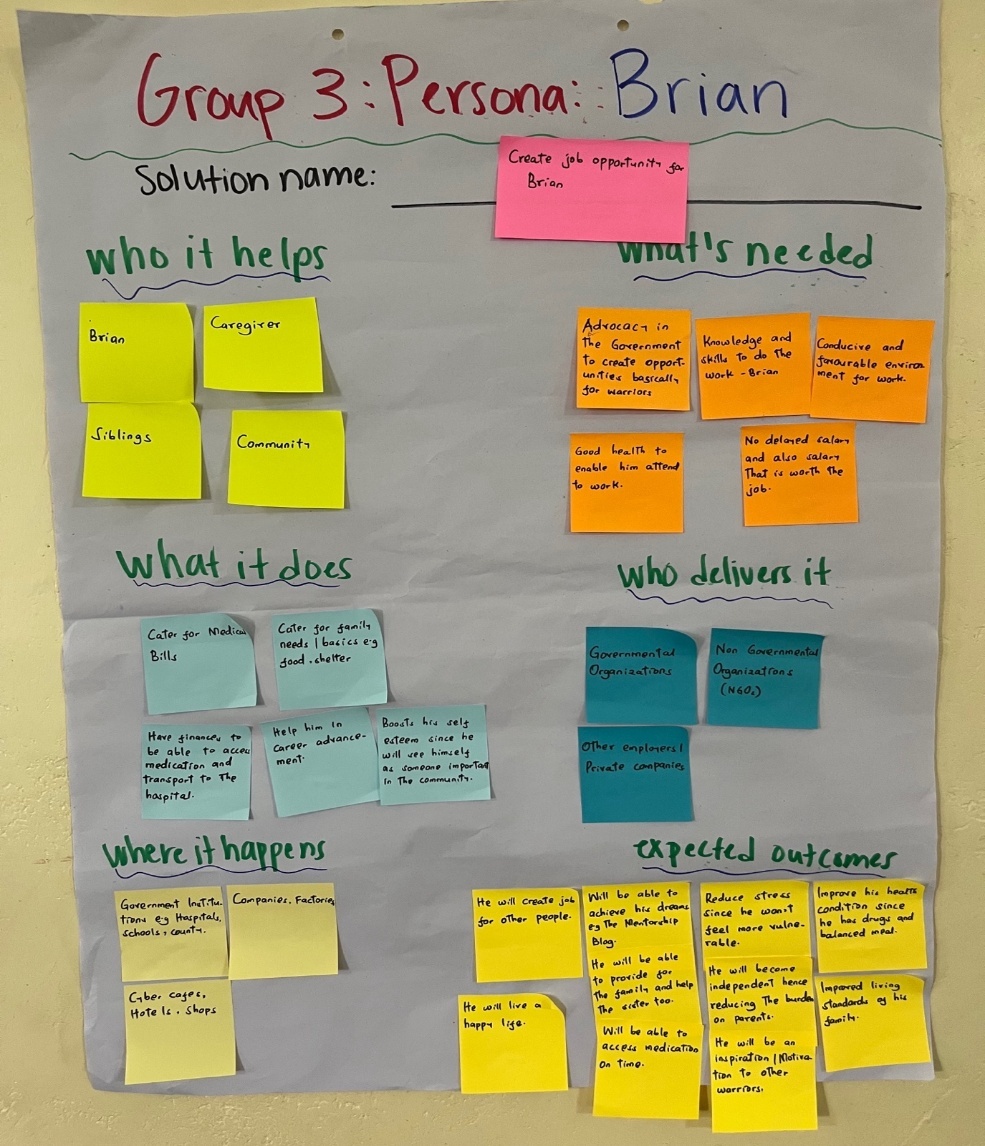
To encourage diverse perspectives and expand the range of insights, each site engaged with a slightly different set of personas. Eldoret included “Aisha,” a sixteen-year-old girl with SCD; “Mama Grace,” a fifty-eight-year-old grandmother and caregiver; “James,” a fourteen-year-old boy navigating school with SCD; and “Nurse Mary,” a provider at the local clinic. Homabay personas included Aisha, Mama Grace, Nurse Mary, and new persona “Brian,” a twenty-two-year-old with SCD. The Webuye workshop included “Mercy,” a fourteen-year-old girl with SCD, “Baba Linet,” a forty-two-year-old father and caregiver, and “Dr. Peter,” a clinician.

Workshop Part 2: From Empathy to Design
Part 2 marked the transition to the Ideation phase of HCD focused on reframing challenges as opportunities.
Ideation and Problem Reframing
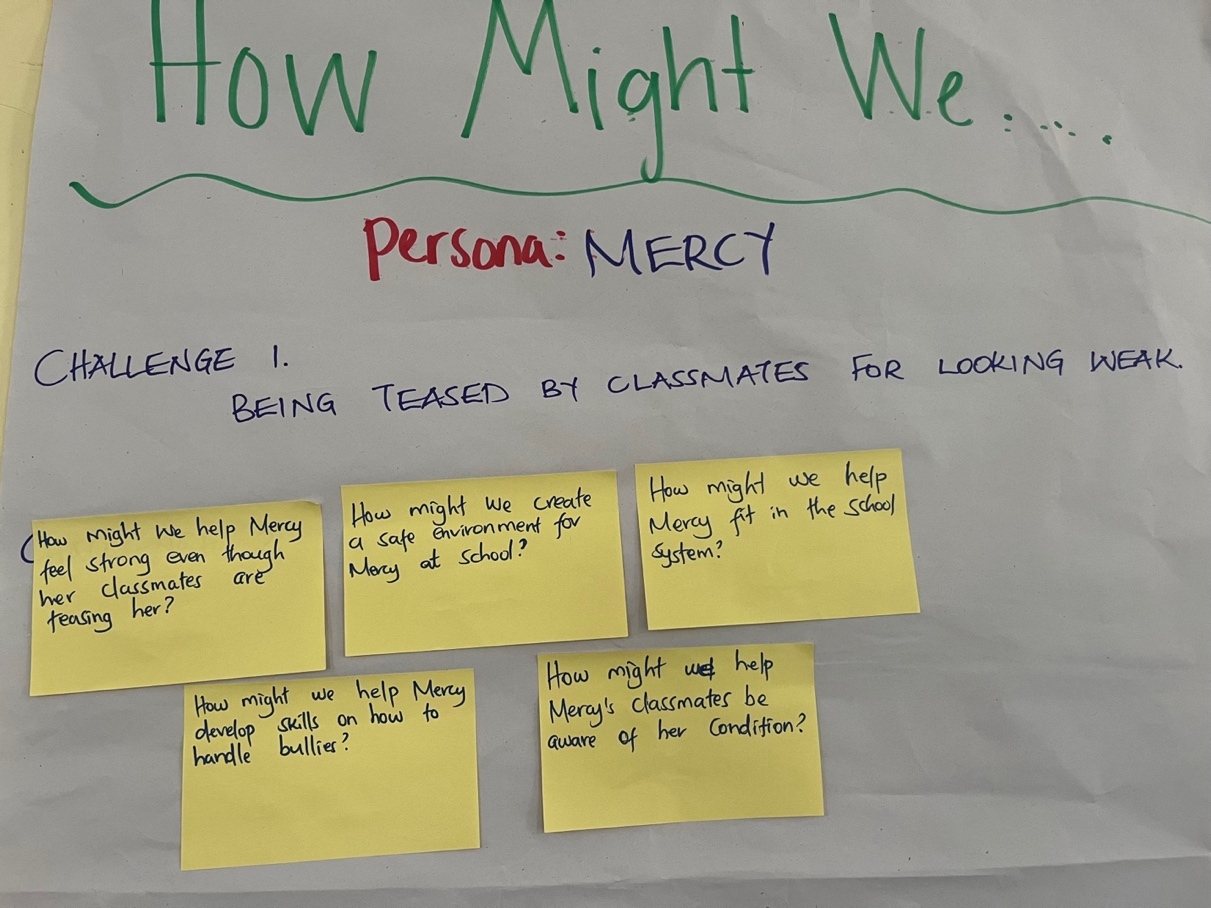
Day 2 opened by linking empathy insights into opportunities for change. Facilitators introduced participants to the “How Might We” (HMW) method, an HCD technique used to transform challenges into open, optimistic prompts for generating solutions (Siemon et al., 2018; Stanford d.school, n.d.). Groups reviewed their empathy maps and identified 3-5 most pressing challenges. These were framed into specific, forward- looking questions such as “How might we improve communication between adolescents and caregivers?” Additional prompts addressed stigma reduction, clinic engagement, and coping support. Questions were posted on a shared wall, and facilitators clustered similar prompts to highlight emerging patterns and shared priorities.

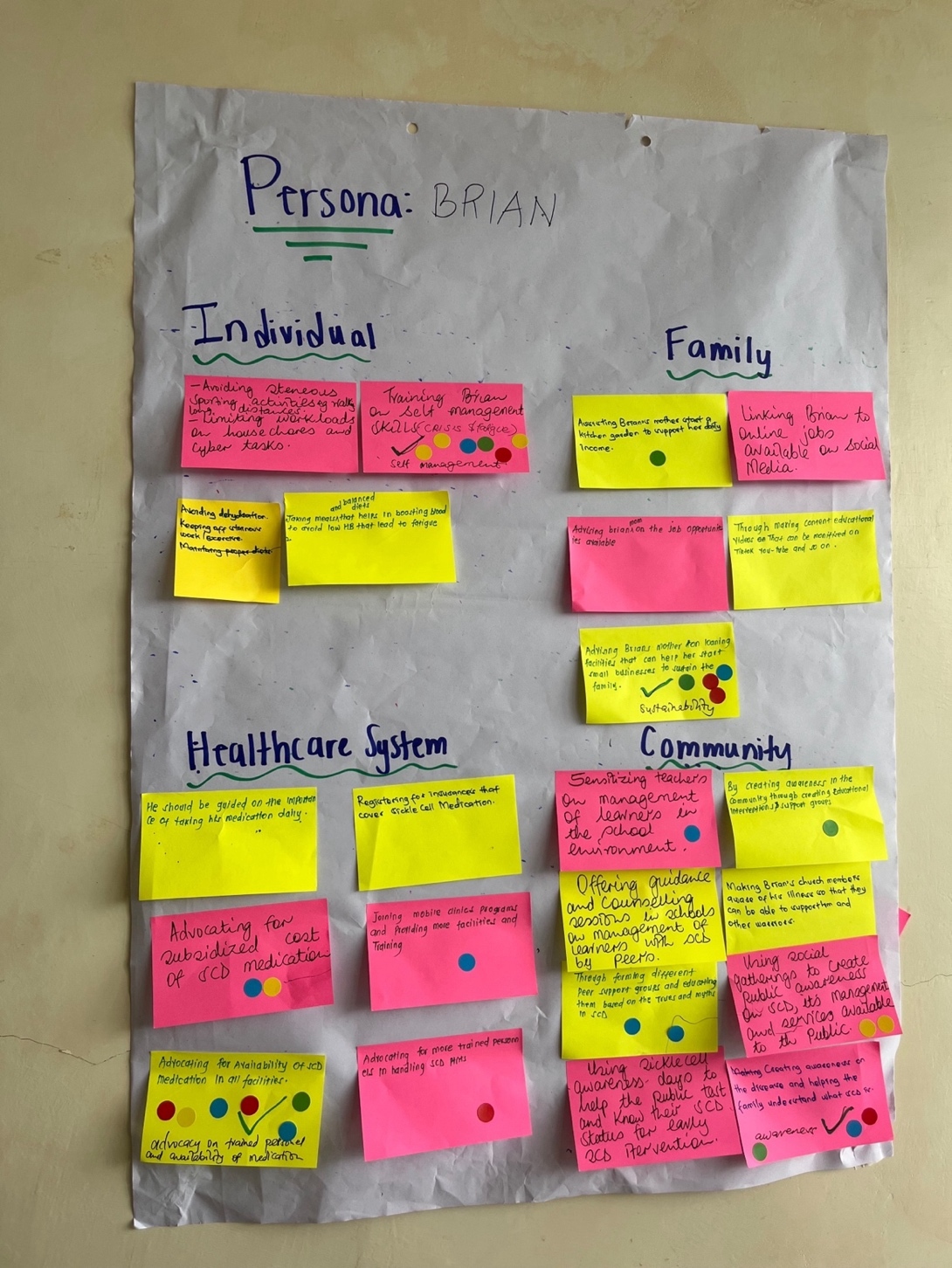
Idea Generation
Next, groups moved into broad idea generation. Facilitators introduced simple brainstorming rules to support open thinking: generate many ideas, suspend judgment, build on others’ contributions, think in both small and ambitious ways, and keep the persona’s lived reality at the center. Participants brainstormed across four system levels: individual, family, community, and clinic. They wrote each idea on a separate sticky note and placed their notes on flip chart organized by system level. The variety of ideas produced was wide, including ideas such as peer mentorship programs, family communication workshops, school-based training to reduce stigma, community awareness campaigns, caregiver support groups, and clinic follow-up strategies. After brainstorming, participants reviewed the posted ideas and clustered similar concepts. This helped reveal where ideas overlapped with others. Facilitators then prompted groups to consider feasibility, cultural fit, and potential reach. Each group discussed which ideas would make the best difference for their persona and selected five most realistic and impactful. Choosing forced participants to prioritize and articulate their reasoning by grounding their decisions in lived experience rather than abstract preference.
Gallery Walk and Community Voting
The room then transitioned into a gallery walk. All flip charts were placed around the room to allow participants to examine ideas generated for other personas. Every participant received five dot stickers and was instructed to place them on ideas they believed had the strongest potential to improve psychosocial wellbeing, regardless of which group created them. This elevated ideas that resonated across stakeholder types. Clusters that received most votes included peer support programs, structured school engagement to reduce stigma, caregiver stress management groups, and predictable psychosocial support within clinics. Groups then strengthened the top-voted ideas by adding practical details. They identified specific activities, who would be responsible, and what resources would be needed. They also suggested adaptations to make ideas workable in rural versus urban settings or across different age groups. Groups reviewed feedback offered by others, creating a back-and-forth refinement cycle which allowed solutions to evolve and helped move the strongest ideas from general concepts toward clearer, workable approaches.

Early Prototyping
Although workshops were structured around Empathy and Ideation, elements of early prototyping emerged naturally. Each group selected two ideas to develop in even greater detail using a structured template. They outlined the purpose, target users, setting, and minimal resources needed. Groups then presented one or two solutions to the larger room and received brief feedback, consistent with HCD prototyping, which tests assumptions and strengthens ideas before formal development begins. This helped clarify unclear components, identify missing steps, and strengthen feasibility. Although full prototyping and testing will occur in the next phase of the project, these early prototypes helped move ideas beyond abstract discussions into concrete starting points for future design.

Reflections and Methodological Lessons
The following reflections emerged from structured team discussion following all three workshops, drawing on facilitator notes, synthesis summaries, and debrief conversations. They represent interpretive takeaways from the facilitation experience.
1. Accessible and Inclusive Design Amplifies Diverse Voices
Visual tools, bilingual facilitation, and structured small-group work supported participation across literacy and comfort levels. For example, caregivers noted that the color-coded reflections allowed them to “speak without speaking,” while adolescents shared that seeing quotes on the slides helped them “recognize familiar experiences.” These design choices demonstrated that accessibility is not an add-on but a core component of participatory methods. When materials are simple, visual, and culturally responsive, participants can interpret findings in ways that are meaningful to them and contribute insights that might otherwise remain unspoken.
2. Interpretation Reframes Power Dynamics
The workshops demonstrated how participatory dissemination can shift traditional researcher-participant dynamics by positioning community members as co-interpreters of data. Participants expanded findings and offered lived experiences that the research team could not generate alone. At the close of Day 2, facilitators invited participants to share reflections with the group about what they had learned, which solutions they prioritized, and what they planned to do differently. One health care provider described a commitment to offering a listening ear and helping families find hope beyond clinical treatment, while another participant emphasized that psychosocial support and medications should work together to improve quality of life.
3. Sustained Partnership and Advisory Roles
Finally, participants expressed interest in remaining involved in the next phases of co-design and asked to serve on the planned Community Advisory Group. One participant at Homabay reflected that “when different minds come together, change becomes possible.” This interest in ongoing involvement reflects that when stakeholders see their insights shaping proposed interventions, they may develop a sense of shared investment in the work that can support long-term collaboration during later co-design and implementation phases.
Limitations
Several limitations of this approach should be acknowledged. First, the workshops were made feasible in part by the AMPATH research infrastructure and longstanding trust relationships between the study team and participating facilities. Settings without similar partnerships may encounter greater logistical and relational barriers when attempting to replicate this model. In addition, the resources required to organize multi-day, multi-site participatory workshops should be considered by teams seeking to adapt to this approach.
Second, questions of positionality warrant attention. The facilitation team included both Kenyan and US-based researchers. Kenyan team members led workshop facilitation and ensured local contextual grounding, while US-based researchers contributed expertise in Human-Centered Design methods and analytic synthesis. Although this collaboration strengthened the design process, it required ongoing reflection on how researcher roles, institutional affiliations, and power dynamics may have shaped participant engagement and interpretation. Related, it is important to recognize that the initial problem framing during the focus group design stage was led by the research team (both Kenyan and U.S.-based) based on prior research and experience. While the team includes clinicians and people with lived experience, a comprehensive co-design model would include community members at this very first stage (Jull et al., 2017; Mental Health Europe, 2023; Mosavel et al., 2019).
Third, while the original focus groups included a large age range of adolescents and young adults living with SCD (10-25), the workshops included only older adolescents and young adults. Therefore, the younger participants were not present to participate in the interpretation of findings or early intervention ideation. Engaging these younger adolescents will be prioritized in subsequent phases, as it will be especially important when developing and prototyping specific intervention materials.
Conclusion
This project demonstrated that dissemination could function as a foundation for collaborative design rather than an endpoint of research. Aligning dissemination with the Empathy and Ideation stages of Human-Centered Design positioned community members as co-interpreters and co-creators of psychosocial intervention ideas. Through this process, participants expanded the original analysis, and generated actionable solutions grounded in lived experience. More broadly, participatory dissemination can serve both as an ethical practice for returning findings and as a practical bridge between qualitative research and intervention development in global health research (Jull et al., 2017; Mosavel et al., 2019). Methodologically, this work illustrates how dissemination can be structured as an early design phase rather than a unidirectional reporting step. The Community Advisory Group will be established and will include workshop participants who expressed interest in continued involvement and will carry this work forward into deeper co-creation, prototyping, and intervention testing.
Funding
This work was supported by the Josiah Charles Trent Memorial Foundation Endowment Fund at Duke University and Charles Lafitte Foundation Program for Research in Psychology & Neuroscience at Duke University.
Acknowledgements
We thank Webuye County Hospital, Homabay County Hospital, and Moi Teaching and Referral Hospital in Kenya for their support and collaboration throughout the study.
Conflicts of Interest
None
Ethics Statement
This study was approved by the Duke University Institutional Review Board (Protocol #2024-0016) and the Moi University Institutional Research and Ethics Committee (IREC/2024/884). Written informed consent was obtained from all adult participants and assent from all minors.
Corresponding Authors:
-
Yvonne A. Ochieng, Department of Psychology & Neuroscience, Duke 27708-0086, USA. 2200 West Main Street, Suite 800, Durham, NC 27705 Mailing address Box 90086, Durham, NC 27708-0086 E-mail: yvonne.ochieng@duke.edu and
-
Eve. S. Puffer, Department of Psychology & Neuroscience, Duke University, 2200 West Main Street, Suite 800, Durham, NC 27705 Mailing address Box 90086, Durham, NC 27708-0086, USA. eve.puffer@duke.edu