Acquired brain injury (ABI) refers to brain injuries not incurred at birth or due to developmental factors and typically excludes degenerative diseases (e.g., Parkinson’s disease, dementia). ABI includes traumatic brain injury (TBI), stroke, tumor, or infection. For many, ABI is a life-altering event. Even years post-injury, a substantial proportion of individuals report negative functional outcomes in the areas of cognition, mobility, behavior/emotion, and activities of daily living (Ponsford et al., 2014). Allied health rehabilitation professionals (e.g., speech-language pathology, occupational therapy, physical therapy, vocational rehabilitation, social work, recreational therapy, neuropsychology) can help to address some of these challenges through therapies focused on participation in daily life (World Health Organization, 2001).
Despite the evidence base for brain injury rehabilitation, there is a well-documented research-to-practice gap (Groah et al., 2009; Lynch et al., 2018) which results in long delays in the clinical uptake of effective interventions. In order to produce knowledge that is more relevant, contextualized, and transferable, researchers may consider collaborating with key end-users (Camden et al., 2015), adopting a practice-based research lens (Crooke & Olswang, 2015), and partnering with clinicians to reduce the power differential (N. Douglas et al., 2023). Furthermore, once knowledge is generated there should be a plan to disseminate beyond scientific publications with involvement of study individuals (Chen et al., 2010). Dissemination within rehabilitation research often remains researcher-driven, text-based, and unidirectional, thus limiting whose knowledge is represented and how that knowledge circulates. Unmasking Brain Injury (UBI), an art-based community project, was already a free-standing and sustainable mode of communication to which ABI survivors could generate and share knowledge of life, priorities, and experiences after ABI. This paper addresses a critical gap in the participatory methods literature by providing an example of conceptualizing and executing participatory dissemination.
In this paper, we detail participatory-focused research conducted across previous studies (Gregory & Kemp, 2024; Kemp et al., 2025). Gregory & Kemp (2024) analyzed how people with ABI express, through art, the emotional experience of brain injury. Kemp and colleagues (2025) found that individuals with ABI use narratives to personally reflect on their journey and to share with others. This work advances the concept of participatory dissemination by documenting how a pre-existing, community-led arts practice (UBI at Hinds’ Feet Farm) co-produces, interprets, and shares evidence with people living with ABI. Through this partnership, creative expression served as both the medium and the mechanism for equitable knowledge translation.
Hinds’ Feet Farm & Unmasking Brain Injury
Hinds’ Feet Farm (HFF) was incorporated in 2000 and provides services for adult brain injury survivors in North Carolina, representing a paradigm shift from the traditional medical treatment model toward a holistic model emphasizing health, wellness, and community belonging. HFF’s mission is to maximize the post-injury potential of individuals living with brain injury through integrated, person-centered programs, allowing them to pursue meaningful activities while developing a sense of belonging at home and in the surrounding communities. HFF offers day and community-based programs in Asheville and Huntersville, North Carolina and two residential homes on its Huntersville farm, currently serving approximately 60 brain injury survivors.
UBI was inspired by the National Geographic (Stone, 2015) article entitled “Behind the Mask: Revealing the Trauma of War”, which highlighted how veterans were guided by an art therapist to create masks illustrating their hidden feelings about their brain injury and its effects (Walker et al., 2016, 2017). HFF members then created their own masks reflecting their lived experiences with ABI and the impacts the injuries had on their lives. This collection of 19 masks created by HFF members was displayed publicly at The Checkered Ball, a fundraiser for HFF, in March 2015. HFF’s founding executive Martin B. Foil III wrote that “guests were mesmerized by the display of masks our members had completed. Throughout the evening, numerous guests were always seen at the display, reading the stories of triumph and tragedy, of despair and hope” (Foil, 2021).
Recognizing the power of this project, HFF sought to expand opportunities for all brain injury survivors, including those outside the organization, to tell their story through art. In June 2015, UBI officially launched with a threefold mission:
1) to promote awareness of the prevalence of brain injury; 2) to give survivors a voice and the means to educate others of what it’s like to live with a brain injury; and 3) to show others that persons living with a disability due to their brain injury are like anyone else, deserving of dignity, respect, compassion and the opportunity to prove their value as citizens in their respective communities (Unmasking Brain Injury, n.d.)
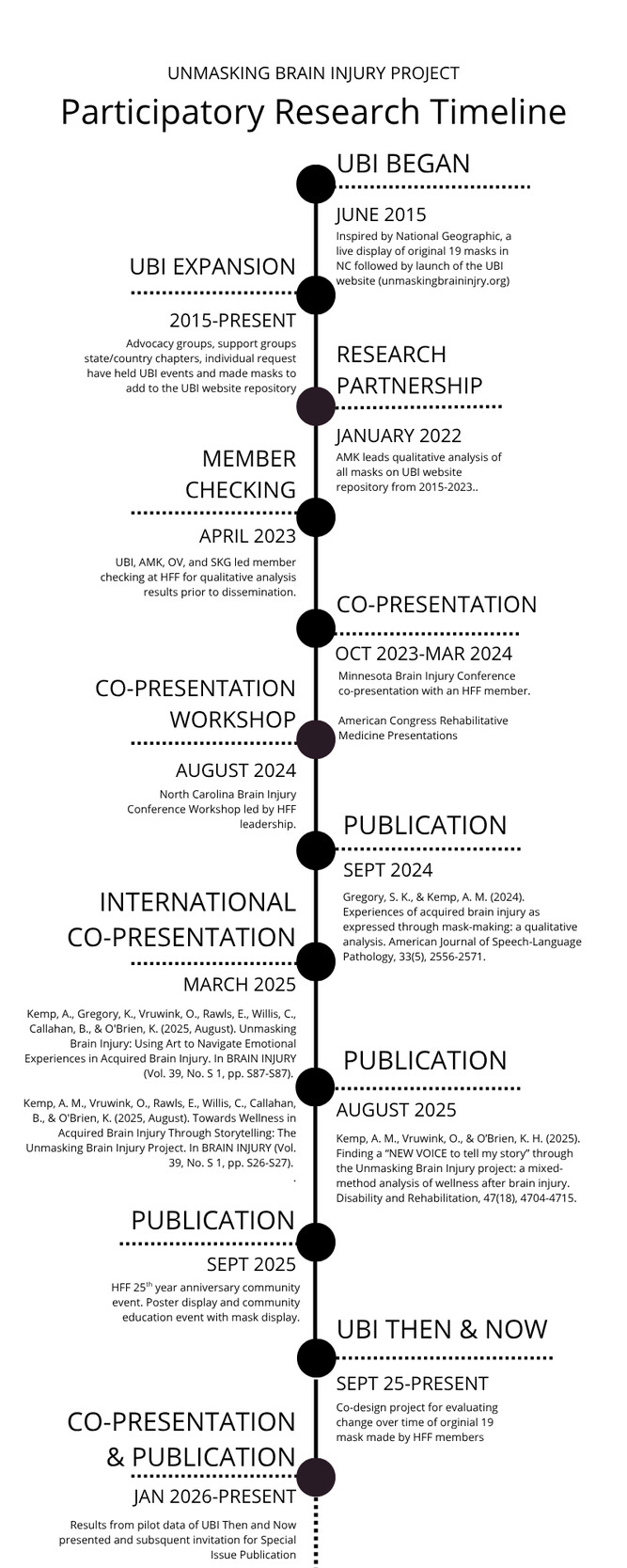
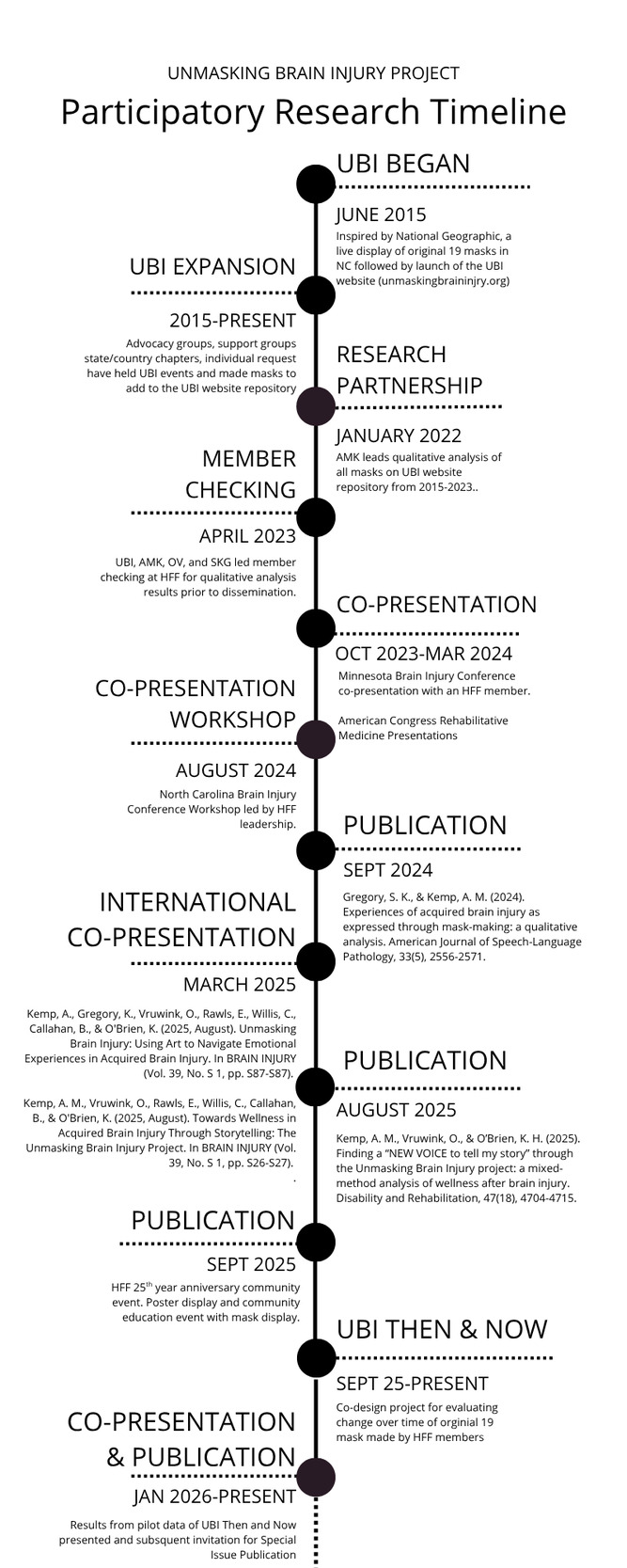
Since its inception, UBI has spread to 40 U.S. states and seven countries, with masks displayed at numerous brain injury awareness and advocacy events. The project currently houses over 1,500 masks on its website, representing a global network of creative advocacy and connection. This underscores how community-driven initiatives can naturally function as mechanisms for participatory dissemination, predating formal research involvement. Figure 1 shows a timeline of UBI and the subsequent integration with academic partners.
Positionality Statement and Reflexivity
All authors identify as White cisgender women. OV and AK are clinically trained speech-language pathologists. OV is a doctoral candidate in Speech-Language-Hearing Sciences, SKG is pursuing a master’s degree in speech-language pathology, and AK is an assistant professor in a Speech and Hearing Sciences Department. ER is a licensed clinical social worker, and CW is a licensed recreational therapist; both work at HFF, are Certified Brain Injury Specialists, and represent community-based practitioner perspectives within the authorship team. As non-academic community partners, ER and CW contributed across all phases of the project, including study conceptualization and alignment with community priorities; facilitation of mask-making and reflection sessions; participant recruitment and support; interpretation of findings within a community rehabilitation context; and co-development of dissemination activities. OV and AMK led manuscript writing with contributing support from SKG. ER and CW also contributed to manuscript writing and editing to ensure that interpretations accurately reflected participant experiences and community values and to support translation of findings for clinical and community audiences. All authors have experience working with individuals with ABI across a range of severities, chronicities, and functional levels.
The research team engaged in regular debriefings to examine how professional training, disciplinary assumptions, and positional authority might shape data interpretation. These reflexive exercises aimed to ensure that the messages people with ABI conveyed through their masks and narratives remained central and that the knowledge produced was grounded in survivors’ lived realities.
Participatory Methods
Methodological Framing
Our participatory approach frames dissemination itself as both a method and an outcome. The stories, artwork, and shared reflections generated through this project functioned simultaneously as data, dissemination, and intervention. Continuous feedback loops between research analysis and community engagement demonstrated how the project co-produced rehabilitation knowledge rooted in creative expression and mutual learning. Additional analytic procedures and extended results that build on these data sources are reported in previously published manuscripts, which address the findings of the described methods (Kemp et al., 2025; Kemp & Gregory, 2024). The following sections describe the participatory dissemination outputs that emerged from this work as a source of information for other academic and community partnerships to consider.
Research Design and Approach
Our research studies (Gregory & Kemp, 2024; Kemp et al., 2025) were informed by a participatory action research (PAR) framework grounded in principles of practice-based evidence. This approach was selected for its alignment with UBI’s long-standing community advocacy and creative expression. Rather than positioning individuals with ABI who created UBI masks at HFF as research subjects, the PAR model framed them as co-researchers whose experiential knowledge shaped all stages of inquiry within these studies through analysis review prior to any dissemination products. Our overarching research question explored how storytelling through art and mask-making supports identity reconstruction, agency, and social connection for people with ABI. Data collection and interpretation were iterative and dialogic, emphasizing reflection, feedback, and mutual learning. This iterative process ensured that evolving insights from artists and community partners directly shaped analytic priorities. In this way, the research remained rooted in community-defined meanings rather than externally imposed frameworks.
This approach diverges from traditional dissemination models that prioritize “evidence-to-practice” hierarchies and unidirectional knowledge flow. Instead, it is informed by an epistemological stance that recognizes lived experience as a legitimate form of evidence capable of informing research design, interpretation, and dissemination. The scope of the PAR model enables researchers to adjust data collection methods and research questions in response to insights gained through community collaboration. Such flexibility allowed the research team to integrate developed themes (e.g., empowerment, tension) into the analytic lens as they surfaced organically through community dialogue. This perspective strengthened the ecological validity and cultural responsiveness of the results. All study procedures were reviewed and deemed exempt from IRB oversight due to the artwork’s public nature and accompanying narratives (IRB #25-0440). Names and identifying features were anonymized or included with explicit permission from HFF for third-party analysis by the authors. Ethical considerations were therefore grounded in shared values of transparency, dignity, and community ownership.
Practice-Based Evidence
Our work directly builds on the ongoing UBI project. After eight years of community-led advocacy through art, we employed a practice-based evidence model to examine how storytelling through creative expression influences identity, agency, and social connection for individuals with ABI. Derived from UBI’s corpus of artwork and stories, we developed a method to evaluate these creative products for insights relevant to clinical rehabilitation. We examined the masks, accompanying personal narratives, and written or recorded reflections using art-based and narrative analytic methods. A preliminary framework for evaluating expressive content was co-developed by clinical researchers and individuals with ABI. This framework was then iteratively refined through member checking with individuals who had previously created UBI artwork. In this way, the practice-based evidence model served not only as a methodological scaffold but also as an epistemic structure that positioned community-generated perspectives as central to interpretation. This approach facilitated theory-building that was grounded in participant-derived meanings and enhanced the validity of the analysis and interpretation of the data.
Member Checking
Member checking extended beyond conventional forms of validation to become a collaborative analytic process. Individuals with ABI at HFF participated in structured discussions and open-ended dialogue that examined how art communicates aspects of identity, recovery, and connectedness in the context of rehabilitation.
These exchanges occurred in accessible community environments and incorporated multimodal supports (e.g., visual prompts, written keywords, assistive communication devices). In line with participatory ethics, facilitators adopted a stance of humility, prioritizing individuals’ own interpretations over clinical or academic framings (Banks et al., 2013). Member-checking sessions used open-ended conversational formats that allowed participants to guide the discussion and introduce issues of personal relevance. Principles of clarification and teach-back were used throughout these dialogues to confirm mutual understanding, reduce interpretive error, and ensure conceptual alignment between participants and researchers. Participants were provided with synthesized summaries of previous discussions and invited to edit or expand on the analytic interpretations. These iterative returns of information strengthened the credibility of the findings and ensured that the emerging framework accurately reflected participant-derived meanings.
Data Collection and Analysis
Data sources included a) the art-based masks and narratives (see Supplementary Materials, Table 1), b) transcribed member-checking discussions and reflective dialogues, and c) field notes and memos from presentations or community exhibitions. The narratives are written descriptions generated at the mask-making workshops, private events, or through personal request to make a mask. In each of these formats individuals with ABI were provided a packet that included instructions on how colors, shapes, symbols, or words can be used to display the lived experience with brain injury. (Readers are referred to unmaskingbraininjury.org for more details or to download the mask-making packet.) Given the variety of settings in which UBI events could be held, the level of support in both creating the masks and the written narratives likely varied to a degree between individuals.
Analysis followed a constant comparative method within an interpretivist framework (Creswell & Poth, 2023). The analytic process cycled through descriptive coding, pattern identification, and theme generation, with each iteration revisited collaboratively by the research team.
Participatory Dissemination Outputs
We conceptualized dissemination in this project as both a product of collaboration and a site of ongoing interpretation. The artifacts, presentations, and publications emerging from our work functioned simultaneously as data and narrative exchange. Through the creative expression of individuals with ABI, traditional dissemination became a process of advocacy, reflection, and shared meaning-making. With our resulting outputs, we aimed to support academic and clinical research practice, as well as survivor advocacy and community and public education on ABI.
Academic Products
Academic dissemination focused on situating creative and experiential knowledge within formal scholarly discourse. Peer-reviewed manuscripts and professional conference presentations documented the participatory framework, methodological decisions, and co-analytical processes that shaped the project (Gregory & Kemp, 2024; Kemp et al., 2024, 2025; Kemp & Gregory, 2024). These findings established a foundation for understanding quality of life, goals and priorities, and areas of growth after ABI. Academic dissemination also kindled cross-disciplinary dialogue by linking arts-based inquiry within PAR into rehabilitation science to inform better care and methods to elicit person-centered perspectives on life with ABI.
At one co-presentation, academic information was presented orally, with embedded videos of artwork and footage of mask-making events. One video featured an HFF member presenting their mask, providing viewers a firsthand voice within the dissemination process. Creative products such as these extended our reach beyond academic and clinical settings, inviting wider audiences to interact directly with lived experiences of recovery after brain injury.
Creative Products
Creative dissemination prioritized accessibility, affective resonance, and narrative integrity across both academic and community settings. Video showcases, professional conference exhibits, and a digital gallery introduced audiences to survivors’ masks and narratives as creative research products. Distinct from scholarly venues, community-based exhibitions were intentionally designed as public-facing, relational spaces that centered survivors, families, and local community members. To celebrate HFF’s 25-year anniversary, the research team traveled to participants’ communities to co-facilitate mask displays and structured conversations about brain injury, recovery, and advocacy. These exhibitions were hosted in accessible community locations and included guided discussions that supported survivors in sharing their stories, educating local audiences, and identifying advocacy priorities relevant to their own contexts. Survivors’ masks and accompanying reflections were presented in multimodal formats that encouraged viewers to engage with lived experiences of brain injury in ways that were emotionally resonant and locally meaningful. By using the artwork as both data and dissemination, this approach positioned creative expression as a form of evidence capable of capturing complex dimensions of identity, recovery, and social participation not easily represented through conventional text-based methods, while also fostering reciprocal dialogue, community education, and advocacy grounded in participants’ own communities.
Shared Platforms
Shared dissemination platforms created opportunities for collaborative authorship and reciprocal knowledge exchange. Researchers and day-program staff members co-authored publications and co-presented at professional and community events. During poster presentations, standing side-by-side allowed both to engage with attendees from both academic and community contexts and to respond to questions through complementary perspectives. Another example of shared platforms included a state brain injury conference workshop. HFF representatives led a mask-making experience for survivors in addition to reporting research findings on quality of life after ABI. In this way, the created art and clinical practice indicators were merged into a shared space for practitioners and survivors. This collaboration enriched interpretive discussions and offered a combined breadth of expertise for situating the work across settings. Through joint approaches in presentations, writing, and reflection, we demonstrate participatory dissemination in practice.
Discussion
This research demonstrates how use of creative, community-led advocacy projects can inform rehabilitation practices. This collaboration exemplifies how to expand traditional recovery models to center lived experiences and bridge the gap between real-world participation and clinical rehabilitation. The UBI project, long established before academic involvement, has produced more than 1,500 masks worldwide as a form of storytelling, advocacy, and connection among people with ABI. When researchers joined this initiative, the goal was not to alter what was already effective, but to learn from and amplify a self-sustaining practice of lived experience. Through this collaboration, creative expression was used to inform rehabilitation practices for people with ABI by translating experiential knowledge into tangible, accessible, and actionable forms. Mask narratives and group discussions highlighted identity disruption, invisible cognitive-communication challenges, and participation barriers not consistently captured in standard assessments. For individuals with ABI who experience reduced self-awareness, the artistic process offered an alternative modality for reflection, often eliciting meaningful insights into how participants understood their own lives, priorities, and recovery goals. Unlike standardized quantitative measures, which may lack contextual grounding for an individual to truly evaluate themselves, the creative process situated recovery within lived experience and personal values. These insights informed clinician and trainee education, supported more person-centered goal setting, and prompted reflection on how rehabilitation can better address identity, participation, and invisible symptoms. Community exhibitions and facilitated discussions further supported advocacy and knowledge translation by helping clinicians, students, and community partners integrate lived-experience perspectives into care and outreach.
This work exemplifies how research can follow rather than lead community expertise, emphasizing reciprocity and respect for existing infrastructures. These findings align with practice-based evidence and community-based practice research frameworks, which emphasize co-learning, mutual benefit, and equitable power-sharing (Corrigan & Oppenheim, 2024; Horn et al., 2012; Marrone et al., 2022). Such partnerships enhance relevance, sustainability, and trust within rehabilitation research (Novak et al., 2021). They also echo evidence from the art-based literature, demonstrating that creative expression fosters belonging and well-being (Jones et al., 2019; Kaimal & Ray, 2017; Mah et al., 2020; Strong & Sather, 2024), while also supporting identity reconstruction and self-awareness, critical for recovery after brain injury (Diaz et al., 2012; J. M. Douglas et al., 2016; Ylvisaker et al., 2008). Including survivors in dissemination products through various platforms (e.g., poetry (Hoepner et al., 2025), storytelling (Strong & Sather, 2024), advocacy-based healthcare presentations (Hoepner et al., 2022)) develops lines to accelerate person-centered priorities into clinical translation.
Recommendations
For clinicians and researchers aiming to develop similar collaborations, several recommendations emerge from this partnership:
-
Engage with existing community programs before proposing research involvement. Co-develop objectives to ensure reciprocity and shared ownership of dissemination.
-
Promote visibility and authorship equity by ensuring people with lived experience and community partners are credited as co-authors, co-presenters, and experts whose insights shape both processes and products.
-
Integrate co-design methods (Vargas et al., 2022) to build interventions reflecting the lived experiences of community members, staff, and survivors.
-
Sustain relationships by prioritizing continuity, communication, and mutual benefit to support long-term impact for both academic and community contexts.
Together, these recommendations illustrate how we used participatory dissemination that honors the expertise of individuals with ABI and the communities that support them. This collaboration between HFF and university researchers demonstrated how academic partnerships can reinforce, rather than replace, existing community wisdom.
Community Partner Reflection
At Hinds’ Feet Farm, the mission is to maximize post-injury potential of people living with brain injury through holistic programs that foster independence, connection, and purpose. UBI began as a way for members to connect with the community, tell their stories, advocate for themselves and others with brain injury, and practice skills in new social situations. In partnering with researchers, the Hinds’ Feet Farm team seeks collaborators who share a commitment to honoring survivors’ voices and expanding awareness of community-based brain injury programs.
This collaboration on the UBI project demonstrated how research, clinical practice, and community engagement can coexist and strengthen one another. The research process encouraged reflection among program staff, reinforced the value of members’ contributions, and introduced new approaches. From the organization’s perspective, publication and dissemination of UBI-related research provide external validation of program impact and help ensure that the perspectives of people living with brain injury are represented in academic and clinical discussions. For staff and members alike, seeing their stories recognized within research contexts affirms that community-based programs contribute meaningfully to broader conversations about recovery after brain injury.
Conclusion
This work exemplifies how participatory dissemination can emerge from community-led practices that invite dialogue and redefine evidence. Through the UBI collaboration, storytelling and art became modalities through which individuals with lived experiences could speak back to researchers and communities, transforming personal artistic expression into shared knowledge and collective advocacy. In doing so, this work demonstrates that when communities author their own narratives in platforms that foster opportunity and purpose, dissemination becomes not a final stage but an ongoing conversation, one that reshapes what is known and who can share it.
Acknowledgments
We extend our sincere gratitude to Hinds’ Feet Farm (HFF) and the Unmasking Brain Injury (UBI) project for their longstanding commitment to advocacy, storytelling, and community leadership. This work would not be possible without the artists, participants, caregivers, and staff whose lived experiences guide and shape the meaning of these findings. We are especially grateful to Martin Foil, Beth Callahan, Janet Guptill, and the HFF program teams for their partnership, collaboration, and insight throughout this project.
We thank the members and caregivers of the Hinds’ Feet Farm Day Programs for their thoughtful feedback during the development, interpretation, and refinement of this work. Their perspectives, grounded in lived experience, clinical practice, and community engagement, strengthened the rigor and relevance of our analysis. We also appreciate the contributions of ARCCH Lab members who assisted with data review and qualitative coding.
Our deepest appreciation goes to the artists and storytellers who created the masks, shared their experiences, and participated in the iterative review process. Their willingness to “speak back” through art continues to inspire ongoing efforts toward participatory dissemination and community-centered research.
Disclosure Statement
The lead academic authors (AMK & OV) participated in member-checking and participatory feedback sessions conducted in person at Hinds’ Feet Farm, for which travel and lodging support were provided by HFF. Two authors (ER & CW) are salaried employees of HFF and serve as leaders within the UBI project. SKG has no relevant financial or non-financial disclosures. All other aspects of the project, including analysis and manuscript preparation, were supported by institutional resources at Washington State University.
Contact Information
Amy M. Kemp, 412 E. Spokane Falls Blvd, Spokane, WA 99202
amy.kemp1@wsu.edu