Background
Suicide is the leading cause of death of children and young people (CYP) in the UK (ONS, 2024) and represents an area of priority for government policy (Department of Health and Social Care, 2023; The Scottish Government, 2022; Welsh Government, 2024). The number of children thinking about and attempting suicide has been continually increasing in recent years (NSPCC, 2020). Children who present with suicidality are generally referred to Child and Adolescent Mental Health Services (CAMHS) for assessment and treatment; however, it has been well documented that CAMHS are struggling to meet demand for their services (NHS England Digital, 2024; Public Health Scotland, 2024a; The Scottish Government, 2018). A recent study investigating two different CAMHS found that 25% of all referrals over a six-month period were for children who had been thinking about or attempted suicide; moreover, there were large differences in how these referrals were being processed, with one area only able to offer an assessment to 31% of these children (Gilmour et al., 2022). Those that were seen by CAMHS did not find the service helpful; children, their parents, and CAMHS practitioners all suggested that CAMHS were unable to offer the type of needs-led and flexible care that they needed (Gilmour, 2021). New ways of working with CYP experiencing suicidality, which are acceptable to them and the people providing their care, need to be developed. Any new model should be designed with CYP themselves.
Treatment models and models of care that are developed for CYP with suicidal thoughts and/or behaviours are generally led by psychologists and/or psychiatrists. Service models are developed by commissioners and service providers, driven by budgets, staff skills, staffing levels, and other resource availability. Service design and re-design within a healthcare setting has predominantly focused upon quality improvement and is typically clinician led. Co-production (working together with people who have experience of the issues) within the context of health services provision is likewise often limited to consultancy and quality improvement. A recent systematic review of co-design/co-production activities with young people in relation to mental health services found that although their voices were being listened to more often, this did not translate into changes being implemented (Sellars et al., 2021). Although some progress has been made to involve CYP in mental health research (Totzeck et al., 2024), CYP with lived and living experience of suicidality are often excluded and considered too vulnerable to participate (Lakeman & Fitzgerald, 2009). However, evidence suggests that participation in research and co-production activities can be beneficial and empowering (Dazzi et al., 2014).
Best practice in co-production means not only inviting people to contribute once the study is up and running, but before the funding application is made at the production/design phase (NIHR, 2021). The Scottish and UK Governments, as well as many other governing and funding bodies now subscribe to the phrase “Nothing about me without me” (Department of Health and Social Care, 2010; Healthcare Improvement Scotland, 2023). This phrase was first made popular by disability rights activists (Charlton, 1998), and now is commonly used to denote that individuals know what they need best and decision should be made with, and not for people. CYP have a right to have their views listened to and be involved in decisions that are about them; this includes both research about them and the design of services they use (UNCRC, 1989). The Scottish and UK Government approach to service re-design also sets out that people using the service are actively involved in the process (Government Digital Service & Central Digital and Data Office, 2012; Scottish Government, 2019).
This pilot project aimed to facilitate the co-production of a research protocol for a much larger grant award which will co-design a new service model for CYP people experiencing suicidality. This co-design will be achieved by working together with CYP, parents, practitioners, service providers, other academics, and policy and decision makers. Our key objectives were to:
-
Engage a wide range of stakeholders with experience or expert knowledge in using, delivering, or providing mental health support services for CYP who have been thinking about or have attempted suicide. This included young people, parents, practitioners, service providers, policy and decision makers, and academics.
-
Facilitate a series of workshops to support these stakeholders to work together with the research team to co-produce a research protocol and provide other means to contribute for people unable to attend the workshops.
-
Host an in-person event to allow dissemination of the key elements of the research protocol as identified by the group and bring people together to support relationship development and collaborations which will support delivery of the future research protocol and on-going knowledge exchange.
This paper begins with reflections from a young person with lived experience of suicide who collaborated with the researchers throughout this project, including writing and re-drafting this manuscript. We then describe the co-production approach undertaken to create the protocol for our future study, before explaining what happened and how things turned out. Our reflections on what went well and the challenges we faced, which are woven through the results, are then briefly summarised. These reflections from the researchers together with those from a lived experience expert provide key insights into working collaboratively with such a wide range of stakeholders, whilst also ensuring a safe and productive workspace for everyone, most especially young people with experience of suicidal thoughts and behaviours.
Reflections from a lived experience expert
The following is a reflective account on the personal experience of one of the young people who participated in the project. Their experience on this project is situated within their previous experiences of co-production work, highlighting the impact of power dynamics, trust and meaningful collaboration.
Reflection
Based on my own personal experiences and those of my peers, I believe that co-production within mental health is plagued by infantilisation. There appears to be a notion that co-production is merely a tick box exercise, just quickly consult those that are directly affected, to say that we have done so, and then not take those views further than the room or video conference call in which they were shared. This is a nuanced issue. Numerous researchers, public and third sector workers often approach co-production with well-meaning intentions and significant will. However, because of various factors such as funding, capacity and planning, co-production ends up in the aforementioned equation. It is a standard impact over intention conundrum, co-production done poorly, no matter how well intentioned, leaves marginalised people feeling frustrated and ironically more unheard than before. Most unfortunately, it often leads to them being less likely to partake in further co-production work.
Good co-production work requires a magic combination of ingredients to create the perfect product. However, ultimately, good co-production is not about perfection. It is about an understanding of power. Infantilisation is common in mental health co-production. The belief that people with mental health issues cannot judge their best interests often hinders the serious consideration and integration of their perspectives. This feels further compounded when the work is concerning young people. Young people throughout sectors are not treated as equal partners in decision making. They are frequently sidelined, and insights dismissed because of preconceptions around their maturity and understanding. True co-production requires that we dismantle these power imbalances, collaborate meaningfully, and consistently recognise the unique expertise of those that have experienced an issue first-hand.
The experience of this project felt fundamentally different from my other experiences of co-production from the outset. In the initial stages, the project was explained clearly and the support available was distinctly transparent. The researchers approached the recruitment stages with intentional and meaningful support and from the beginning. The level of thought around the distribution of power was remarkably clear in initial conversations. I never felt concerned that this was a tick box exercise for the researchers in their project. Our contributions, as CYP with experiences of suicidality, were at the forefront and given the appreciation it deserved in project design.
The workshops themselves felt equal and non-hierarchical. This was clearly largely facilitated by the researchers’ significant efforts. This was not a lucky result; it was clear the researchers had considered deeply how to create such a space. Pre-conceptions and personal internal biases often hold back much of co-production. What made this project so different was that it was starkly clear that this was not the case for the researchers. In the workshops, it felt that they wanted to know what people’s views were, not merely have us agree with the researchers’ opinions. The researchers valued everyone’s views and contributions equally, regardless of their age, experience, or position.
However, it is impossible to avoid CYP’s natural apprehension to such environments, where you are giving opinions informed by often difficult experiences. The mix with third/public professionals was useful, but even amongst their peers, CYP can have difficulties. Regardless of this, the researchers created the best possible environment they could. I believe this was largely rooted in the strong trusting relationships the researchers had developed with the CYP. They knew all our names; we had relaxing and personable conversations at the start. Something that stood out was that support was never an afterthought; it was always at the forefront. Various forms of outreach were used. This was extremely valuable and made me feel more supported and valued than I ever have in any other project. Ultimately, the researchers created a comfortable and friendly space in an affirming and non-condescending way. CYP were treated equally to their “older” and “professional” counterparts with care and sensitivity to our more specific needs.
For me, the event was the standout aspect of the project. The hierarchy of power felt completely inverse from the norm. CYP and our views were the focus of the event, and we were involved and integrated into the event in ways that worked for us on an individual level. This again was created by the researchers’ meaningful and intentional efforts. The researchers regularly checked in with us throughout the day and I could sense we all felt valued. The researchers went the extra mile with the event, literally giving the CYP a platform on their own terms.
Overall, my experience of this project shows that trust, equality, and intentionality in power distribution are critical to effective co-production, especially when involving suicidality and young people.
Methods
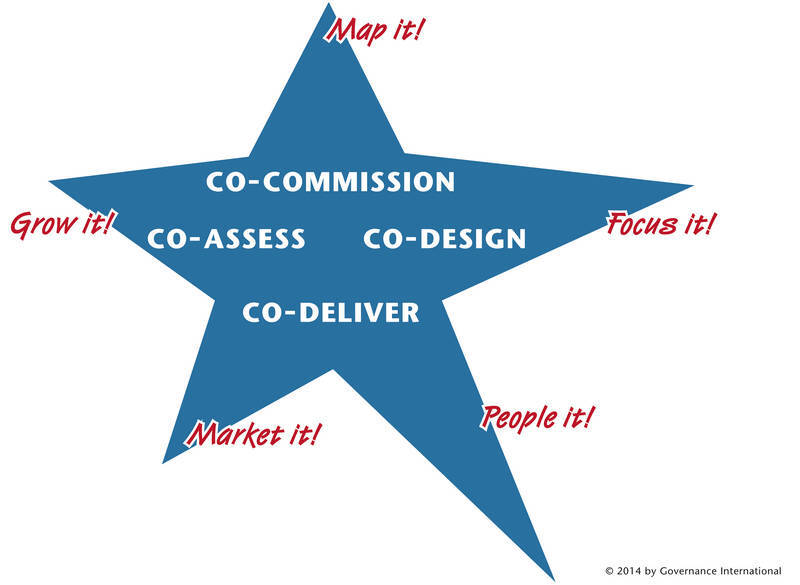
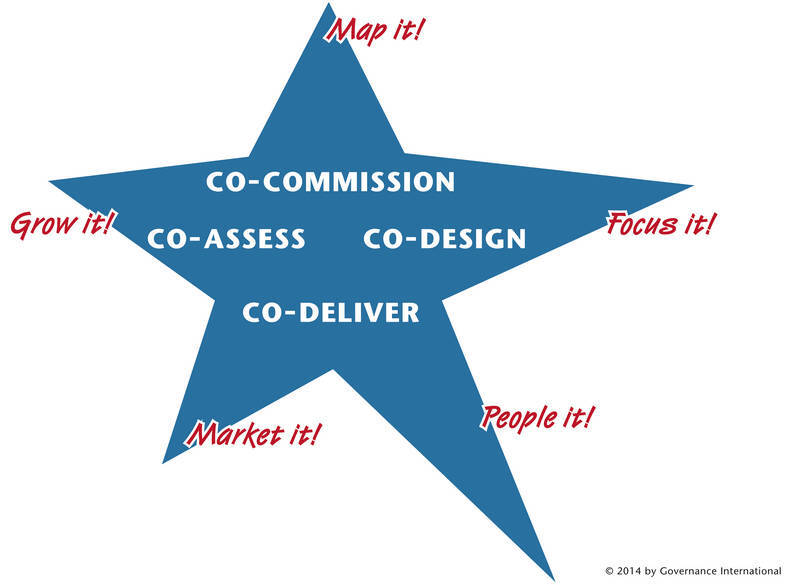
There are many models of co-production and co-design now emerging (Messiha et al., 2023) and it is important to ensure that the approach taken best fits with the task and people involved (Carr & Patel, 2016). The NIHR advocate use of the six principles of co-production approach to research which should guide co-production activity in research (NIHR, 2021). These principles emphasise engaging people in reciprocal relationships, sharing power, including all perspectives and skills, respecting and valuing the knowledge of all those working together on the research, and joint understanding (NIHR, 2021). Additionally, the co-production star (Figure 1) is a model that has been used successfully across many UK, and international projects (Governance International, 2019). It provides a model for co-production that can readily be applied to service design and development and can be used together with the five principles of service design.
As this project was concerned with co-producing a research protocol for a future service co-design project we aimed to:
-
Map it – Map existing forms of co-production and ways we can harness learning around mental health support services for CYP that have been thinking about or attempted suicide. This involved identifying pre-existing groups that work with CYP in this context, so that we could learn from work that has already been done or is on-going.
-
People it – invite young people with experience of suicidality, and practitioners from these key organisations to contribute to the discussions and protocol creation.
-
Focus it – Focus the group on the task of considering what the aims of the future research study should be, the co-production approach it should take and the overall study design.
-
Market it – Present the study protocol together with the people involved in creating it, to potential funders, and organisations that might be interested in delivering the new service model.
-
Grow it – Invite participants and other stakeholders to register their interest in joining a future co-production advisory group. Make an application for a substantial grant award to co-design a service model.
The practicalities of engaging with and bringing together CYP with experience of suicidality with a wide range of different stakeholders, was based on the lead researcher’s extensive experience of working with CYP experiencing suicidality both as a practitioner and researcher, as well as good practice guidance for working with/involving CYP in research (NIHR, 2021) and specifically CYP who have experienced suicidality (Webb et al., 2024).
Recruitment
Recruitment occurred over two months between October and November 2023. It was important the workshop participants represented as many key-stakeholder groups as possible. This included CYP with experience of suicidality (12-25 years), parents (not necessarily from the same family), youth mental health practitioners, service providers, policy makers, and academics who have experience or expert knowledge of providing or using mental health support services for CYP presenting with suicidality. This study aimed to host a group of 6-10 young people, 6-8 practitioners, and 1-2 parents. We did not want there to be more adults in the group than young people. Drop out was anticipated, and we did not expect everyone to be able to attend all meetings.
The professional stakeholders were recruited through established contacts and networks. The young people were identified through a closed recruitment drive via existing networks and purposive snowballing sampling techniques, targeting organisations known to promote and support involving young people in research such as Children in Scotland, See Me Scotland, Fast Forward, Venture Scotland, and the TRIUMPH Network. By conducting a targeted recruitment to organisations that specifically support marginalised or disadvantaged groups such as LGBT Youth Scotland, Intercultural Youth Scotland, and Who Cares Scotland we hoped to include the voices of young people who may be marginalised or are seldom heard.
Following first contact with an organisation/known expert, JC initiated an online meeting, to introduce themself, explain the project, and answer any questions. They were asked: 1) if they were working with CYP with experience of suicidality that may want to participate in the project, 2) if they were working with CYP with experience of suicidality and they themselves wanted to participate as a practitioner, and 3) if they knew of relevant people, organisations, or groups that they could share the study with to help recruit practitioners and CYP with experience of suicidality. Young people identified as being interested in the project were then offered an online, in-person, or telephone meeting, depending on their preference, to meet with JC and hear more about the project. They were invited to bring along their worker, friend, or family member to support as required. Young people were asked to nominate a safe adult that they were happy for the researchers to contact on their behalf if there were any worries or concerns for their wellbeing that arose throughout the project. JC contacted this person beforehand to make them aware of the project and their role should the young person need additional support. All participants were asked to complete a consent form prior to the workshops and were provided a resource sheet outlining various mental health organisations and resources.
Gift vouchers were offered to CYP as a thank you for their time if they attended workshops, and data allowance for attending online meetings was also made available. Additionally, if the young person needed additional support from their support organisation (typically third sector/charitable organisations) to enable them to participate (i.e., a support worker meeting with them pre- or post-meeting and/or attending the meeting with them) financial recompense was made available to the organisation. Transport costs were available for those attending the in-person dissemination workshop at the end of the project.
Before and after each workshop a researcher “checked in” with the CYP attending, to go over what to expect, any worries/concerns they had, and then post-workshop to see how they felt and offer the opportunity to de-brief. This was done via email or video call, depending on the young person’s preference. JC also maintained contact between workshops with all participants (including practitioners) via email and text messages. Dedicated drop-in times were provided where anyone who wanted to ask for a call or live chat to discuss anything in relation to the project could check in.
Workshops
Three online, 90-minute workshops were delivered to co-develop the research protocol and facilitate collaboration between CYP, mental health practitioners, and academic staff, as they can be more inclusive than in-person meetings. In preparation, LG and JC developed a facilitation guide for the workshops to support consistent delivery, productive collaboration, and the achievement of the study goals. The workshops were scheduled to be roughly one month apart in November (2023), December (2023), and January (2024). Online opportunities have been found to be more appealing for people who are often underrepresented in research (Horrell et al., 2015). Additionally, young people are often dependent on others for transportation which may inhibit participation for in-person workshops (Braun et al., 2017; Fox et al., 2007); as such, hosting these workshops online allowed us to recruit a geographically diverse group of participants (Tuttas, 2015). Research also suggests that online focus groups, as compared to those in-person, may help facilitate conversations around sensitive topics such as suicidality and self-harm (Adams et al., 2005).
The content of the workshops was planned around the life cycle of a research project (Farrimond, 2013). We began by spending time getting to know each other and established ground rules for working together. We then began by introducing the group to the research design process (Farrimond, 2013) and co-create with the group the problem we sought to address and what the overall research question, aims, outputs and impact of the future project could be. We also considered how we should involve CYP, and other stakeholders in the co-design process. An outline of the topics covered in each workshop can be found in Table 1.
There are specific considerations that need to be made when undertaking focus group research and/or coproduction with CYP, particularly in relation to developing comfortable environments that address the power imbalances in researcher/participant and adult/young person relationships (Fox et al., 2007; Thabrew et al., 2018; Webb et al., 2024). This was addressed by having a time for introductions and an icebreaker at the start of each workshop, where first names were used by adults to create an informal environment and the value of sharing power in co-production re-iterated (Fox et al., 2007; Thabrew et al., 2018). Participants at the first workshop were invited to co-create ground rules promoting the emotional safety of the group where issues such as making and dealing with disclosures, expectations around participation, and ensuring everyone used jargon-free language. See Table 2 for a summary of the co-created group guidelines. These were then revisited at the beginning of the subsequent workshops and the in-person event with the opportunity provided for additional points to be added. It was envisaged that the young people would attend the same workshops as the adults and that a respectful, reciprocal, jargon free ethos be established within the group, and if numbers of the group allowed, they would be split into smaller break out rooms to promote discussion.
The workshops were co-facilitated by two researchers: LG led the sessions and has almost 20 years’ experience of working with vulnerable CYP in various roles and contexts including CYP who have had thoughts about or previously attempted suicide, and a further 8 years’ experience involving and producing research with CYP who have experience of suicidality. JC had established supportive relationships with all participants prior to the workshops and has previous experience of facilitating workshops with young people and working with vulnerable populations.
Survey
As a supplement to the online workshops, and to offer additional ways for individuals to participate in a way that was comfortable to them (Davey et al., 2019), online qualitative surveys were developed in relation to discussions held at the online workshops and were sent alongside brief workshop summaries so that participants were able to add to the on-going conversation. . These were employed as a means of gathering rich data that were accessible to a geographically diverse population, unobtrusive, quick, and not burdensome, as the survey could be done at the most convenient time and place for the individual (Braun et al., 2021).
These were made available to anyone who was interested in participating but could not attend the day/time of the online workshop or where they indicated that this was their preferred mode of engagement. Survey data was collected via ‘survey monkey’, with one to three open-ended questions to allow people to share their views and experiences in their own words, without too much restriction on their answers. An outline of the survey questions can be found in Table 3.
Protocol Co-Development: A Logic Model
Following each workshop, a short summary of the key points from the discussions was created, incorporating any additional points from the online surveys. These were then shared with members of the group to give them an opportunity to check for accuracy as well as an aide memoir for the next session, and update for those unable to attend. Prior to the final workshop researchers used these summary documents to populate a logic model (W.K. Kellogg Foundation, 2001), as this helped to illustrate the research journey and break down the key components such as problem, resources, methods, outputs and impact. The logic model was then shared amongst members of the group to consider, before being discussed and further edited at the dissemination workshop.
Dissemination Workshop
The dissemination workshop was planned together with participants from the online co-production group, and they were invited to lead presentations and discussions. This event was held in-person, with lunch provided, and travel expenses available. This was an opportunity for the researchers and co-production group to share their experience of the development of the model, get feedback and input from a wider range of stakeholders on the research protocol, as well as explore their views and their own approach to co-production.
Outputs
The main output from the project was intended to be a research protocol that could be developed for a larger funding application. However, it was also important the learning from the project was shared amongst the network of organisations and individuals that had supported and contributed to the co-creation of knowledge, and therefore a lay summary of the project was also created to be shared. We also wanted to create a level of public awareness about the project and worked with the University of Stirling Communications team to create a short video.
Evaluation
At the close of the in-person dissemination event, we asked attendees to complete a short evaluation form consisting of two open-ended questions: 1) ‘How was the event?’, and 2) ‘Do you have any other comments/suggestions?’. It also asked the individual if/how they would like to be included as this project progresses, offering the following options: 1) ‘Keep me informed’, 2) ‘Intervention Development Team Member’, and 3) ‘Co-Investigator’. If they did, they were asked to offer a contact email address.
Ethical considerations
Although formal ethical approval is not required for public engagement activity (NHS Health Research Authority, 2025), we gave careful consideration to all ethical issues and followed best practice guidance and legislation in relation to consent, confidentiality and the handling of personal data. All CYP were provided vouchers as a token of thanks for their time. We also notified the University of Stirling General Ethics Committee about our project, who confirmed ethical approval was not required for this activity.
Results and Reflections
Researcher reflections on the strengths and weaknesses of our methodological approach to co-production are outlined below. Specifically, we reflect upon the recruitment and engagement of the participants, the planning and undertaking of the online workshops and supplementary surveys, the dissemination of findings, and the co-development of the research protocol.
Participants
In total, six CYP and seven practitioners signed up to participate in the online workshops. Attendance at the workshops varied due to personal availability (shown in Table 4 below), although we maintained communication with all participants via email and teams calls to the conclusion of the project.
Though demographic data collection was not specifically included in our study due to low numbers (Public Health Scotland, 2024b), we were able to recruit CYP with a range of ages (15-25 years), genders, ethnic identities and support needs, from different locations across Scotland. Additionally, we were able to recruit practitioners from four discrete youth support/mental health organisations, as well as NHS practitioners from three different CAMHS sites across Scotland.
Having a researcher dedicated to recruitment, supported this process enormously as there was a single point of contact for organisations and young people. The straightforward, colourful recruitment materials helped (Supplementary file 1), but meeting with practitioners to introduce the project was key in assuring them of the research team’s experience, knowledge, approachability, and sensitivity to the needs of young people with experience of suicidality. Establishing trust with practitioners helped avoid gatekeeping, often encountered in research with vulnerable groups (Kay, 2019). Additionally, offering young people the opportunity to meet or have a telephone call to discuss their involvement prior to participation was vital. This allowed the researcher not only to set out what to expect, but chat through what their needs might be, create an individual well-being plan and establish a connection which could facilitate group participation. Founding this relationship also allowed for ongoing support throughout their engagement in the project, with regular contact via text and phone calls, as well as offering time for one-on-one conversations if needed.
Workshops
Discussion
The atmosphere of the online workshops and discussions was a strength of our study. As JC had the opportunity to meet with the CYP and practitioner participants one-on-one (or with a support person if desired) prior to attending the workshops, the participants had a familiar person who they had already begun to develop a positive and supportive relationship with. This, in conjunction with the positive, conversational, and jargon-free tone adopted by the researchers and agreed-upon by the practitioners, aided the creation of a cooperative, judgement-free, and supportive work environment. Furthermore, the co-development of a Group Agreement in the first workshop helped to establish a collaborative environment from the start of the project.
Since our group included both CYP (Children and Young People) and adult practitioners, we were keen to create a collaborative and non-hierarchical workspace where power was shared equally among all participants. To help achieve this, we used smaller ‘breakout’ rooms for discussion sessions, each facilitated by a researcher. These smaller settings helped create a more relaxed atmosphere, making it easier for participants to engage in focused, meaningful conversations. We also encouraged CYP participants to share their breakout group findings with the larger team, promoting inclusion, empowerment, and validation for everyone involved.
Although there was lots of time spent preparing the participants before the workshops, to ensure that they felt as safe and comfortable as possible engaging with the topic, listening and contributing to group discussions, we received feedback following our first workshop that one young person had found parts of the session difficult. The researchers reached out to the young person, first by email and subsequently in a one-to-one meeting. They shared with the researchers that they had found a point raised in the large group discussion about difficulties young people can experience accessing support from CAMHS had resonated with their own experience, but they hadn’t felt able to express their views or experiences due to CAMHS practitioners being present. The young person spoke about how they didn’t have any previous experience of using Microsoft TEAMS/On-line platforms for meetings and this type of forum was new to them. They reflected on positive things they had enjoyed about the meeting but said they would have preferred a young person only space.
The researchers recognised the validity of this participant’s experience and, while ensuring anonymity, brought the suggestion to the wider team, reaching out to the young people individually to ask if there was a preference for a young person only group. The responses from the other CYP indicated a preference for having mixed groups of CYP and practitioners. They expressed that they felt it was important for practitioners to better understand the experiences of CYP with suicidal thoughts or behaviours, and that they were hearing this from the CYP themselves. Empowering and validating the voices of CYP experiencing suicidality is of key importance, as they can often feel a lack of agency throughout the help-seeking process (Gilmour et al., 2019).
To accommodate and validate the desires and feelings of all CYP involved the project, methodological flexibility was required. It is vital to emphasise that participation is completely voluntary and support the participant to engage in ways in which are appropriate for them. In this instance, online surveys presented a more appropriate means of participation for this CYP participant.
Following the first workshop, the researchers received feedback from a practitioner that there was a lot of information for the participants to process in the first workshop. We adapted the researcher presentations for the subsequent sessions to further enhance the accessibility. Finally, despite testing the video-calling software being employed, we encountered some technical problems when attempting to separate the group into breakout rooms for smaller-group discussions during our first session. This was unfortunate, and a hazard of on-line working to be anticipated, however, it did disrupt the session slightly and we worked to ensure it could be avoided for future sessions.
Debrief
For half an hour after each workshop, the liaison researcher offered a drop-in debrief session, where CYP could speak to the researcher via an online meeting or phone call and discuss any worries or things that had come up after the workshop. Debriefs or check-ins were also offered throughout the project. Though not frequently accessed, CYP would often respond to the email which offered a debrief, communicating that they were well/did not feel the need to chat anything over, which allowed for a form of check-in. It was considered of prime importance to offer a space of support, even if it wasn’t needed, and helped to ensure CYP felt supported.
Scheduling the Workshops
As observed in Table 2, there was a slow decline in workshop participation as the project progressed. While some drop-off of participation is to be expected, the notable drop in practitioner attendance may be related to the scheduling of the workshops. To accommodate CYP attending school, university, and scheduled daily activities, our workshops ran in the evening between 5:30-7:30pm. Though somewhat anticipated, asking practitioners to contribute their free time in the evenings (and without the voucher incentive, as offered to the CYP) presented challenges; work commitments, care responsibilities, and the disinclination to attend a workshop after a day of work, appear to be key barriers to retaining practitioner engagement. Additionally, the scheduling of the workshops in November, December, and January may have been an especially busy time for both CYP and practitioners, contributing to the drop-off of attendance at the workshops. Despite these challenges, the continued engagement of CYP (ranging from 50-100% CYP attendance across the workshops) was positive, and, in part, indebted to the consideration of scheduling the workshops at appropriate and accessible times for them.
Surveys
Participation in the online surveys was generally low. The first survey had three responses; the second had four responses; the third survey had zero responses. Notably, engagement in the surveys was most successful when the survey was directly sent to individuals the researcher had been in contact with and had had the opportunity to hear about the project, but were unable to participate in the workshops, as well as participants who had attended the workshops but were unable to attend a specific one. This, as well as the lack of engagement via advertisement on the Participation Network, indicates the value of offering individuals the opportunity to hear and ask questions about the project to encourage engagement. It is important to note that no incentive was offered for completion of the surveys which may also have impacted engagement.
Dissemination Workshop
Attendees
We engaged a range of relevant and interested stakeholders as part of our dissemination workshop. Representatives attended from two Child and Adolescent Mental Health Teams (CAMHS), the CEO of Penumbra, the National Suicide Prevention Lead for Scottish Action for Mental Health (SAMH), See Me Scotland, Fast Forward, Who Cares Scotland, Suicide Cultures (University of Edinburgh), Edinburgh Napier University, and University of the West of Scotland, among others.
Presentations
Three of the CYP participants in attendance presented on our findings from each workshop. They had worked in cooperation with JC to prepare their presentation as per their preferences. For one participant, they asked to be supported to help write a script from which they could present. The other two participants preferred to work from the summaries of workshop discussions (which were distributed shortly after each workshop) and checked in with the researcher if they needed support or guidance. Again, a personal and person-centred approach to supporting the CYP was important. The researcher was available to support the CYP before their presentations and throughout the day. In the evaluation form completed at the close of the workshop, the CYP participants noted that they felt the event and presentations were a success and that there was a lovely atmosphere. They valued the opportunity to be listened to and to listen to other people. Additionally, they appreciated being able to meet the wider co-production team in-person for the first time.
Group Activities and Discussions
After the presentations, participants and attendees were invited to consider and suggest improvements to the logic model that had been developed. Participants were provided a hand-out of the logic model and were asked to discuss it in their small groups and write any comments or suggestions on a post it note and place it on a large poster print-out of the logic model. Another poster offered a space for comments and suggested that may not be related or fit neatly onto the logic model. This activity was successful in capturing a range of views, experiences, and expertise, and offered a means of individuals adding comments anonymously if they did not want to voice them in their group.
After a break, a CYP participant led an open discussion with all the attendees to explore the necessity, value, and challenges of co-production in research. The CYP participant presented statements and preconceptions about co-production and welcomed comments from the attendees; they facilitated discussion with the attendees and managed insights from multiple perspectives. This activity was entirely CYP-led and generated fruitful and challenging discussion and raised attention to the often-nominal co-production activities commonly employed in research.
Protocol Co-Development: The Logic Model
Following the online workshops, the research team summarised and analysed the findings to develop a logic model, mapping the journey from the research aims to its outputs and impact. This was distributed to participants via email for member-checking, though there was not a significant response. For future member-checking, it would be beneficial to designate more time and space for an additional workshop specifically focused on exploring and adapting the logic model. These shortcomings were, however, off-set during our in-person dissemination workshop.
As part of our in-person dissemination workshop, we asked our participants and attendees to examine, interrogate, amend, and comment on the logic model. They were provided hand-outs of the logic model and asked to write any comments or amendments on a post-it note and stick them to a large poster print-out of the logic model. This was a valuable evaluation activity, offering insights from a range of stakeholders from various disciplines. We were offered suggestions regarding the range of CYP participants should be recruited in future study to co-develop a service that was appropriate for a range of backgrounds and experiences. It also offered input into additional research activities and directions that could be employed to fully address our research questions and aims. Additionally, it indicated the importance of considering ways in which our research outputs could be evaluated to ensure effectiveness and quality. These comments were incorporated into our logic model.
The co-development of this research protocol, both with the study participants via our online workshops and wider network of stakeholders and experts at our in-person dissemination workshop, offers a clear direction for future research. It outlines: 1) the problem, 2) the research question and aims, 3) research activities, 4) research outputs, 5) research outcomes, and 6) impact.
Evaluation
Participants were invited to complete an evaluation form at the end of the in-person dissemination event and workshop. Overall feedback was overwhelmingly positive, referencing the importance of the research, the style of the event, and the people involved.
Many attendees noted how important and valuable it was to be doing research in this area and with this focus. Regarding the event itself, the space and atmosphere was described as friendly, safe, and supportive. Attendees noted it was very engaging and informative, offering important insight and offered benefit to a range of fields. Discussions were described as thought-provoking and honest. Emphasis was placed on the value of hearing about and discussing co-production; some commented that, while the employment of co-production in research and other disciplines is encouraged, they do not often hear first-hand accounts about organising and participating in co-production activities.
Another success noted by the attendees was, the range of people included in the study and dissemination workshop. It was considered especially valuable to have CYP included in the project and dissemination of findings. Additionally, having attendees from a range of backgrounds and disciplines was considered beneficial to discussion, and offered opportunities for networking and connecting with individuals working in similar fields. Many attendees reached out to offer their support for the research, indicating ways in which they could help (i.e., support recruitment of marginalised CYP for interviews, etc.). Developing relationships and collaborations to support delivery of the future research study had been a key aim of this project.
As a methodological approach, co-production activities and research projects have been criticised as they are not evaluated for their effectiveness or impact (Ali et al., 2022; Staley, 2015). An oversight of this project was not building in formalised feedback and monitoring throughout the project, although experience also tells us that responses to questionnaires at the end of each session may have been less meaningful than the informal feedback and discussions we had with participants. Leaving the evaluation forms to the end also allowed participants to reflect on their involvement in the entire project (if they had been involved throughout). Although we received positive comments and feedback from project participants who had been unable to attend the in-person event, it would have been helpful to have captured these more formally.
Strengths and Limitations
This study was novel in its approach, as stakeholders are often only involved in research after it has been funded and the study commences. This is serves as a good example of collaboration at the study design stage. There is also a dearth of research where children and young people with experience of suicidality are involved beyond the role of research respondent, and we have evidenced that despite concerns about risk, this can not only be achieved, but experienced positively by those involved. A strength of this paper is the inclusion of co-author IM’s reflections on their involvement of the project. However, we also wish to acknowledge that it would have been preferrable to extend this offer to other CYP, but, as is often the case in academic research, paper writing takes place following completion of the funded study; therefore, we were unable to provide the follow-on support and resources needed for this. The careful planning and engagement approach taken throughout this project required dedicated researcher time. Future co-produced research should incorporate sufficient time as well as continued access to finances to compensate people fairly for their time to enable this.
Although we had initially intended to recruit parents to the co-production group, we were unsuccessful prior to the first group workshop. At this workshop we asked those attending whether this was something we should urgently address; however, the young people strongly expressed that although parents’ views are important and they should be consulted, they should not be in the same space as young people as their voices can often be more dominant and inhibit young people from freely expressing their views. This is something we built into the design of the protocol for the future study, but the absence of parent views in this study remained.
Another limitation was that we did not seek permission to use direct quotes from the evaluation forms and informal feedback we received in publications such as this. For future research activity requesting this by prior consent would be recommended.
Conclusions and Recommendations
The co-production approach adopted in this protocol development project allowed young people with experience of suicidality to not only contribute their views and ideas, but also to take ownership of the project and share power with the researchers and other stakeholders. A key strength of this approach, and clear recommendation for researchers undertaking co-production work was the informal, one to one relationship’s established with the young people before the group workshops began, as well as providing lots of opportunities for on-going check ins with the researchers throughout. The feedback and learning from all the participants in this project will directly inform and strengthen the approach undertaken to co-design the new model of care and offers transferable insights for all intergenerational and multi-disciplinary co-production projects more broadly.