There remain ongoing calls for the integration of qualitative methods to improve understandings of care experiences within health services research (Palinkas, 2014). Undergirding these calls is the recognition that qualitative approaches can uniquely strengthen health systems by providing a deeper understanding of traditional quantitative explorations. Accessing the experiences of health service stakeholders (i.e., recipients, providers, etc.) not only provides insights into how these systems are embodied but also identifies where and how changes can be effectively implemented, translated, and adapted (Long & Jiang, 2023). When these intersectional insights, concerns, and perspectives are mobilized to improve health systems, the legitimacy, credibility, and acceptability of these proposed improvements are bolstered (Recchia et al., 2022).
We extend these appeals for an increased use of qualitative methodologies, also including a commitment to adopting participatory approaches. Participatory approaches have been identified as a means to transform the health service systems relevant to the communities we engage by “dismantling social and structural barriers between participants and practitioners/researchers” (Kitzie et al., 2020, p. 1). Although diverse in their methods, participatory research is theoretically grounded in the belief that people’s life experiences, positionality, and intersectional identities produce different forms of knowledge that are important to solving complex social ills (Aldrich & Marterella, 2012; Benjamin-Thomas et al., 2021). In recent years, the World Café (TWC, Brown & Isaacs, 2005) has been employed as an example of a participatory method suitable for addressing these social ills. Given its adaptable nature to both contexts and participants (Kinney & Kinney, 2024), TWC has been successful in accessing and connecting diverse and multiple stakeholder groups across the healthcare landscape (Kavanagh et al., 2020; Mamo et al., 2024; McGrath et al., 2023; Murphy et al., 2020), especially when used in tandem with other data collection approaches (Alunni-Menichini et al., 2023).
The purpose of this manuscript is to illustrate how TWC methodology was adapted for a conference setting and employed as a strategy to address commonly reported challenges in participatory research broadly, and with research participants who interface with racially minoritized disability communities. Scholars have identified enduring issues including recruitment and retention, establishing trust, superficial participation of stakeholder groups, power hierarchies and unequal decision-making, as well as the need to balance rigor with inclusivity (Cornish et al., 2023; Johnson et al., 2025; Lake & Wendland, 2018). Specific to the study example presented here, we address the challenges of (1) recruitment and retention of provider partners, (2) data collection timelines that were dependent on the funding cycle, (3) integrating or reconciling transdisciplinary practices, and (4) flattening power hierarchies (Cornish et al., 2023; McGrath et al., 2023; Shiele et al., 2022).
World Cafe Methodology
As a participatory methodology, the World Café (TWC) is grounded in the belief that those within an identified community already possess the knowledge and creativity to address the issues impacting them. The method mobilizes this belief to collectively and collaboratively access and facilitate community knowledge, generating critical thought and, when strategically leveraged, critical possibilities for action. TWC aims explicitly to do this by including as many community members as possible (Löhr et al., 2020). The method is also beneficial when these members are meeting for the first time, particularly during an in-depth exploratory phase that lasts at least an hour and a half (Brown & Isaacs, 2005).
Guiding Principles
TWC seeks to access and mobilize diverse community thought and action through activities that are guided by the following seven principles: 1) setting context; 2) creating a hospitable space; 3) exploring questions that matter; 4) encouraging everyone’s contribution; 5) cross-pollinate and connect diverse perspectives; 6) listen together for patterns, insights, and deeper questions; and 7) harvest and share collective discoveries (Brown & Isaacs, 2005, pp. 55, 70, 87, 102, 112, 127, 140). These guiding principles are unpacked below.
Fundamentally, TWC is rooted in prompt-guided, small-group conversations that occur in an environment conducive to naturalistic conversation (Principle 2). After being introduced to the parameters of, and establishing ground-rules for, the “café” (Principle 1, 2), community members split into groups of four to five people. Each group is then given a previously established, open-ended prompt (Principle 3), and asked to discuss in relatively unstructured ways. Discussions typically occur in three, twenty- to thirty-minute rounds. These small groups then fragment and reformulate into new small groups, encouraging the sharing of and building upon ideas with different community members who are present in the space (Principle 4, 5).
While groups reformulate, a host remains behind to serve as a bridge between the previous and new conversations. This host may stay the same throughout the entire process or change with each cycle; what matters is that the bridge between groups is maintained. In addition to sharing key insights after a TWC rotation, hosts are encouraged to ask open-ended questions, invite those who have not yet contributed to do so, and offer opportunities for reflection (Brown & Isaacs, 2005). Democratically, it is not necessary to train a host in advance—anyone attending a TWC can, and is encouraged to, serve in this role (Brown & Isaacs, 2005). At its core, “hosting is really about being yourself rather than just playing a formal role” (Böjer, 2005, p. 156) in an effort to create a welcoming environment.
While a host serves as a bridge, the remaining community members continue to interact in novel combinations as a means of engaging in collaborative knowledge generation, transfer, and evolution. Ultimately, this cross-pollination enables the collective experiences and perspectives of the larger group to become clearer (Principle 6). This clarity can be supported through iterative large-group discussions and reflective summaries, or by creating visuals that represent both small and large group discussions (Brown & Isaacs, 2005). Although there are no prescriptive guidelines for recording the collective discoveries that emerge through TWC (Principle 7), data are primarily qualitative and often take the form of visual data (e.g., film, tablecloth drawings, exhibitions), audio recordings and subsequent transcripts, and note taking by participants or hosts (Kitzie et al., 2020; Löhr et al., 2020; Pettican et al., 2021).
The Importance of Conversation
In addition to its participatory orientation, TWC is shaped by living systems theory. A living systems theoretical framework contends that within a complex network of actions, symbiotic relationships exist between individuals (Baird-Wilkerson, 2003). It further asserts that non-linearity, uncertainty, and adaptive self-organization are building blocks to change (Wells & McLean, 2021); thus, TWC brings together groups of people with different life experiences to discuss common interests (e.g., occupational therapy, healthcare, equity) and produce otherwise unanticipated outcomes and new knowledge (e.g., new partnerships, actionable initiatives, topics to be explored). It is because of living systems theory that a conversational nature is distinctly crucial to the successful implementation of TWC.
Although prompts initially structure TWC conversations, the resulting content of these real-time conversations and the way they unfold are not controlled by facilitators (Brown & Isaacs, 2005). Conversations, however, are primarily shaped by the rationale for convening the café, who participates, and the parameters for their participation. The preparatory structuring of the conversation’s context in this way facilitates a more natural, and free(er) flowing discussion, which is ultimately the method’s desired outcome.
How is it Useful to Health Services Research?
TWC’s ability to reveal the network of relations between participants establishes it as a meaningful method for exploring and understanding health services encounters in multifaceted ways. From a logistical perspective, TWC allows for the rapid collection of data from a large number of people. Although this advantage is not unique to TWC, these strengths are complemented by the method’s strategic leveraging of its democratic, conversational, and relational nature which facilitates the "[noticing of] a deeper living pattern of connections at work in our organizations and communities’’ (Brown & Isaacs, 2005, p. 4). In other words, TWC is a representative microcosm of the community it represents. The method is structured to bring together people with a shared commonality while honoring their diverse positionalities, experiences, and practices in ways that they otherwise may not have been able to interact or in such a timely manner. What this means for a more nuanced study of health services encounters is that, after a discussion has been framed around a prompt, TWC’s participatory orientation not only allows participants to share their most meaningful experiences more casually but also enables those experiences to be novelly riffed upon by others in the space.
The conversational nature of this sharing in TWC effectively primes participants to corroborate or contest their healthcare engagements. In turn, health services researchers are provided with examples that are both rich with nuance and emblematic of patterns across participants’ experiences and positionalities. This effectively generates representative data that spans the spectrum from individual to collective experiences, enabling researchers to gain expedient insight into the structural and moderating influences of health services. Although TWC has been successfully applied to health services research across practitioners and disciplines (Recchia et al., 2022), its application in conference-like settings remains emerging (e.g., Kavanagh et al., 2020; Wilson et al., 2017), and little methodological guidance or examples on how to adapt TWC for this site remain scarce.
Using TWC as a Data Collection Approach in CPAR: A Study Example
In the following example, we aim to both further cultivate TWC’s potential for data collection at professional conferences and improve the health services’ ability to gather stakeholder perspectives and understandings of service provision to support CPAR projects. Before presenting the example study, we provide the positionalities of the researchers involved and the study’s research objectives. Next, we present the description of the example study. The example study is organized by TWC’s guiding principle which include 1) setting context; 2) creating a hospitable space; 3) exploring questions that matter; 4) encouraging everyone’s contribution; 5) cross-pollinate and connect diverse perspectives; 6) listen together for patterns, insights, and deeper questions; and 7) harvest and share collective discoveries (Brown & Isaacs, 2005, pp. 55, 70, 87, 102, 112, 127, 140). Principles are also captured in each section’s header.
The example study is presented in this way to highlight how each principle was implemented and adapted in the hopes of offering more guidance for those interested in developing and conducting a TWC. This style of organization also allows for quick reference and identification of specific principles, while also offering TWC’s gestalt when read in its entirety. We then discuss TWC’s limitations and the lessons the example study provided the research team, before offering concluding reflections.
Researcher Positionalities
The authors represent some of the academic research partners in the study example, including an early-career investigator and mentor, and two doctoral-level students. The first author identifies as Black and female. The doctoral student researchers identify as white, with the second author identifying as male and the third author as female. We hold entry-level degrees in occupational therapy and have received formal education in occupational science. Our intersectional identities of difference have undoubtedly influenced our interests and participation in action research with multiply marginalized communities, including the theoretical positions we have adopted and research designs through which those positions/constructions are applied. Most prominently, the first author’s recurrent experiences of anti-Black racism and other systems of oppression against the mobilization of ethnic and gender minoritized people. The second author is situated within this study’s work through his scholarship–informed by his position as a queer person–on socio-political theories of change and their relationships to structures of power. The third author’s self-reflexivity and scholarship on white racialization and whiteness ideology inform her orientation to this study.
The Example Study’s Research Objectives
The following TWC took place as a part of a larger CPAR study that aimed to (a) better understand the structural factors, particularly structural racism, that impact healthcare access and utilization for minoritized people with IDD, and (b) enable the development of enhanced, consumer-provider informed pathways to health. The first four meetings of the CPAR study convened with Black research partners with IDD and their care partners and were exclusively dedicated to identifying the contextual characteristics that influence access, and mapping the individual characteristics, contextual characteristics, and health behaviors that influenced their care. The fifth meeting with community partners involved, in part, preparation for TWC to gain input and feedback from community partners on the questions that would be presented, building on initial insights gleaned from the study. Hence, the first several meetings of the CPAR directly informed what was discussed during the portion of this study that used TWC. The last five meetings of the CPAR were dedicated to integrating provider research partners into study discussions to reveal differences in perceptions of care access between each cohort, before collaborating to develop an anti-racist model of support to improve access, service delivery, and enhance community assistance.
As will be demonstrated, TWC not only served as a bridge to increase recruitment opportunities among provider researcher partners (i.e., occupational therapy practitioners attending a state association conference) but also allowed for the preliminary exploration of their perspectives as the second phase of the study approached. Even more critically, TWC aided in revealing their experiences as occupational therapy practitioners within a broader community of service providers and how their collective experiences were mediated.
Principle 1: Setting Context
TWC method was utilized to structure an oral presentation for the annual fall conference of the North Carolina Occupational Therapy Association. The annual conference convened over two days on a college campus centrally located in the Piedmont region of the state, and consisted of continuing education opportunities including pre-conference institutes, short courses, poster sessions, roundtable discussions, vendor exhibitions, assistive and adaptive technologies competitions, and more.
Participant Demographics. The conference session was attended by a total of 23 participants, comprising occupational therapy practitioners (n=12), occupational therapy educators (n=5), and occupational therapy students (n=6), including one pre-occupational therapy undergraduate intern. Five of the 23 attendees were racialized as Black. All other attendees identified as white. Six of the attendees, including the second author, identified as male, while all other attendees identified as female. These demographics are similar to those reported in the most recent survey on diversity in the occupational therapy profession in the United States (i.e., 4% of practitioners identify as Black or African American, and 91.1% of practitioners identify as female) (American Occupational Therapy Association [AOTA], 2023). Relatedly, these observations can be made of occupational therapy in North Carolina (Lombardi et al., 2024). All attendees were employed or matriculated through an occupational therapy academic program in the state. On-site recruitment, consent, and data collection procedures were approved by the Office of Human Subjects Research and Institutional Review Board at the University of North Carolina at Chapel Hill. All TWC attendees who remained throughout the conference session received a $25 gift card in appreciation for their contributions.
TWC as a Conference Session. The conference session was advertised as a “works in progress” presentation to potential attendees. The submitted abstract indicated that the presentation would share preliminary findings from the larger CPAR study, as described above—with an emphasis on sociocultural and anti-racist implications for occupational therapy practice—and involved a notice of consented participation in roundtable discussions using TWC, which would ultimately contribute to the study’s aims. The formal objectives of the presentation were to: 1) explain the role of CPAR practices in advancing inclusive and emancipatory action; 2) describe the impacts of structural and contextual barriers on access and utilization of health services for Black people with IDD; and 3) identify the ways through which occupational therapy practitioners may contribute to the reproduction or amelioration of barriers to access and utilization of health services.
The presentation was divided into four phases. The first 30-minute block was dedicated to describing the larger CPAR study, preliminary findings, and the role of CPAR in enhancing inclusive research towards transformative action for Black people with IDD. This block was followed by TWC with a sequence of 1) a 15-minute block for large group discussion, 2) a 30-minute rotating roundtable discussion, and 3) a final 15-minute large group summarization and analytic discussion. Informed consent was formally provided before the discussion portion of the presentation, and attendees were able to rescind consent and excuse themselves from the conference session at any point. Throughout the large group discussions and subsequent small group discussions, three graduate assistants, including the second and third authors, documented key words and phrases to aid data collection. Additionally, these research assistants served as each table’s “café host” to reiterate TWC prompts, encourage participation, and provide summaries and key insights. All group discussions were audio-recorded and transcribed verbatim for analysis as recommended by Schiele and colleagues (2022).
Logistically, it is important to note that slight adaptations to TWC protocol (i.e., not utilizing café-like decor such as tablecloths as documentation tools and modifying discussion time) were made to accommodate the constraints of a conference session (Bumble & Carter, 2021). As described later, the study also adapted TWC procedures by using audio recordings during both large and small group discussions. This particular deviation from typical TWC protocol allowed for enhanced analytic rigor and ensured the context of participant statements was retained (Shiele et al., 2022).
Principles 2 and 3: Creating a Hospitable Space to Explore Questions that Matter
As noted in Principle 1, the conference presentation began with an in-depth explanation of the larger CPAR study, including specific contextualization of the approach’s ability to identify and dismantle traditional power hierarchies that prioritize academic and researcher expertise over the experiential knowledge of attendees. The first author further explained the importance of creating a “communicative space” for session attendees; that is, all attendees would commit to engaging in dialogue to clarify their concerns and observations as it pertains to structural determinants (i.e., structural racism) of health and how race-based disparities in healthcare may be sustained and reproduced through occupational therapy practice, noting conceptual links between the discussion prompts for TWC and the aims of the larger CPAR study.
TWC Session Overview. TWC began with a brief explanation of its methodological intentions and principles. The first author discussed the specific procedures of the roundtable discussions and introduced the three graduate students serving as café hosts at each discussion table. Large group discussion was facilitated by providing all attendees with opportunities to ask clarifying questions before signing the consent forms. Following consent procedures, attendees collaboratively established conversational ground rules (e.g., mutual respect, trust, etc.) and how they would be applied to the ensuing dialogues. During the initial 15-minute large group discussion, attendees were asked to define and share their perspectives on what it meant to be healthy, to be unhealthy, and their definitions of equitable healthcare. Before progressing to the small discussion groups, the first author facilitated additional dialogue among attendees to achieve consensus on how the group characterized health and ill health, as well as the group’s shared definition of health equity.
TWC then transitioned to previously arranged tables for small group discussions. Once situated, the café hosts presented the following prompts:
-
In what ways might occupational therapy practitioners influence the health of Black people with IDD?
-
What do you consider to be facilitators to health for Black people with IDD? Consider your local environment including practice setting and community assets (e.g., community resources).
-
What do you consider to be barriers to health for Black people with IDD? What role does occupational therapy play in eradicating those barriers?
Prompts used during the presentation were informed by responses to individual semi-structured interviews and focus groups conducted with research partners with IDD and their care partners (e.g., about what they believe providers should know, what [un]health means for them, how their experiences have influenced these perceptions of health, and an ideal service experience including what needed to be accomplished for it to exist) during phase 1 of the larger CPAR study.
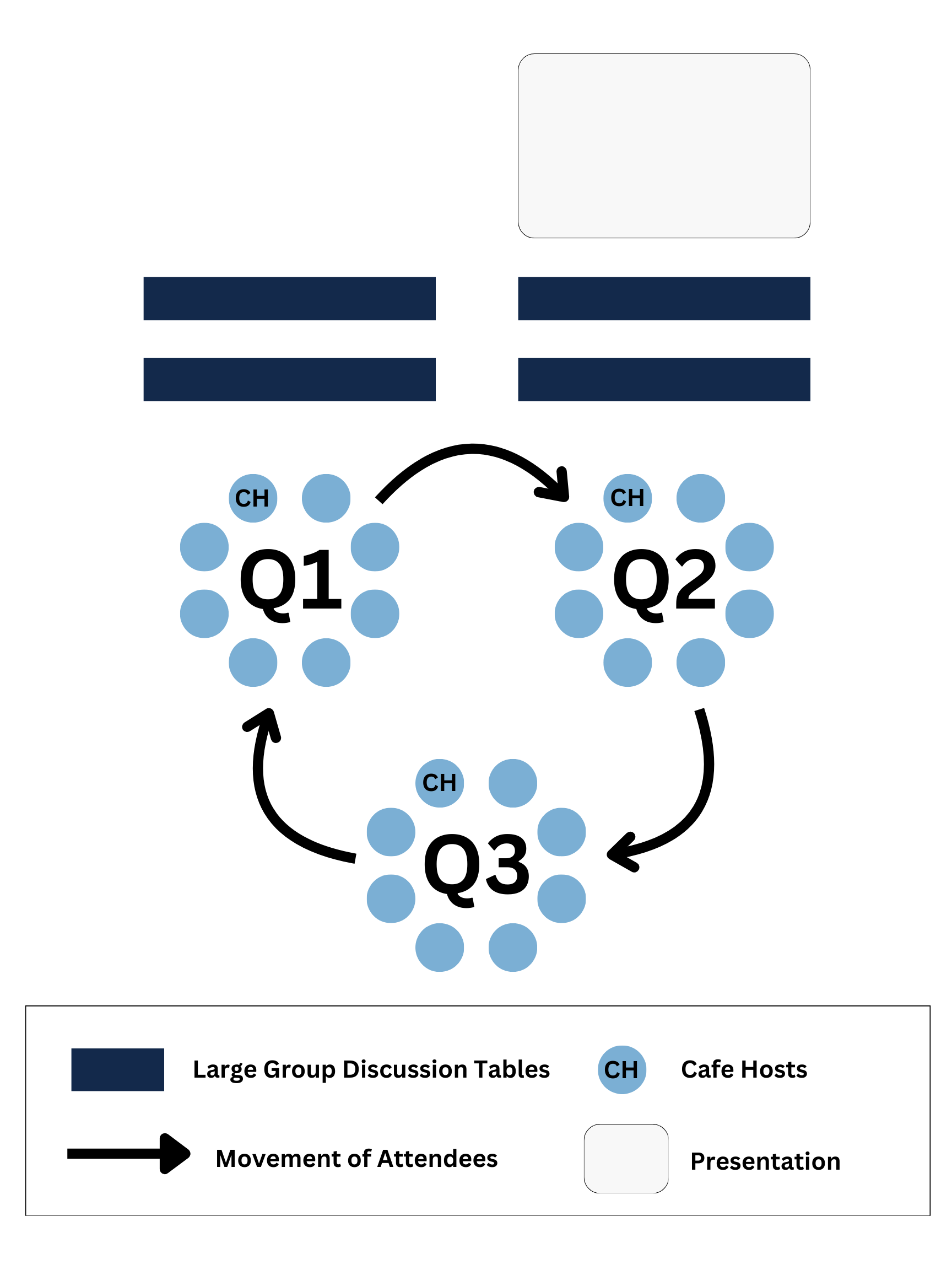
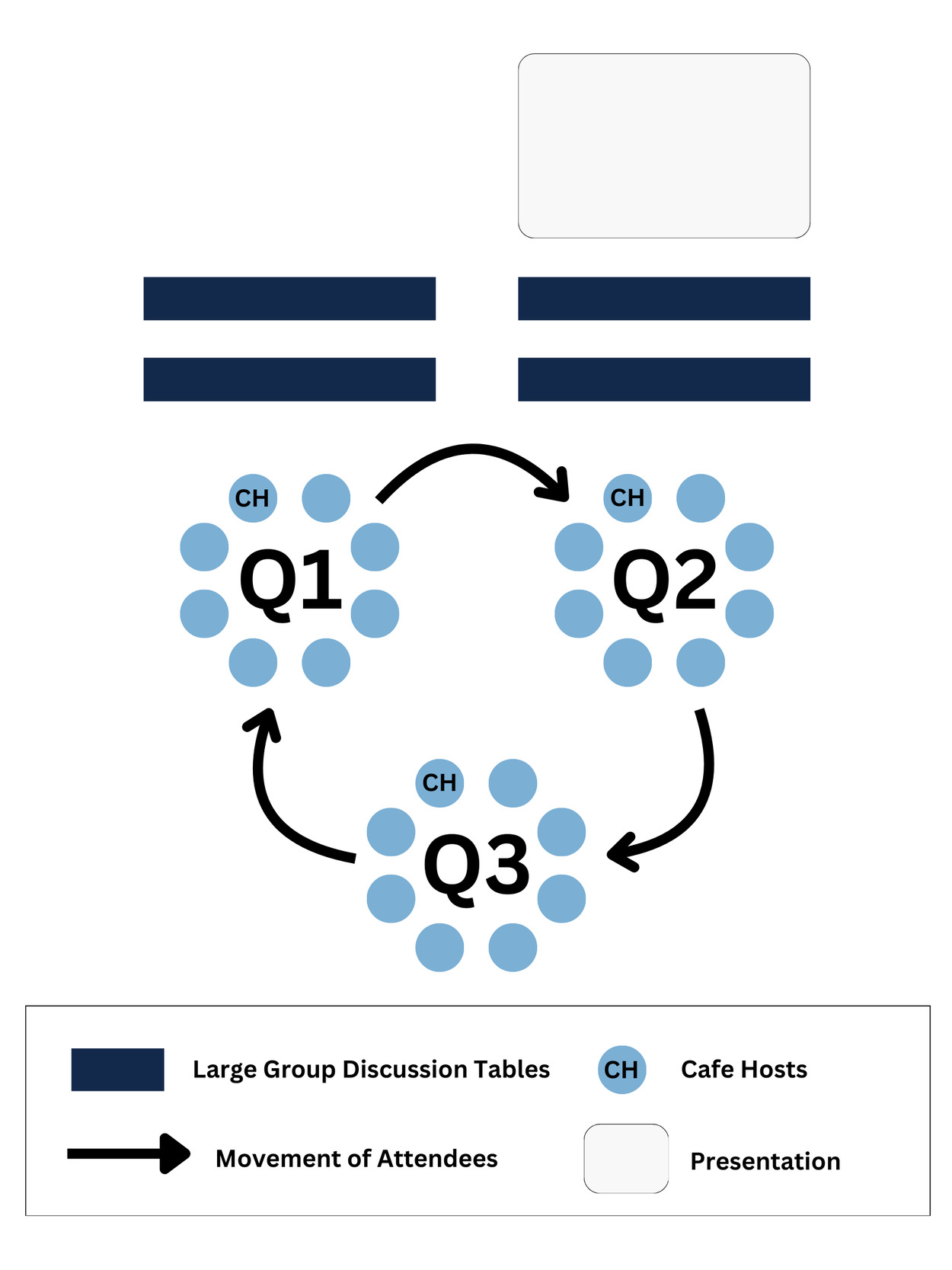
TWC attendees rotated through each question once at 10- minute intervals for a total of 30 minutes, while café hosts remained at their designated table throughout the small group discussion period. Figure 1 depicts the approximate setup and movement of attendees. At the start of each rotation, café hosts summarized what was discussed by attendees in the previous round. This allowed each new group to corroborate and/or contest discussion points by relating themes to their own personal and professional experiences and beliefs (Brown & Isaacs, 2005; Shiele et al., 2022).
Principles 4 and 5: Encouraging Everyone’s Contributions and Connect Diverse Perspectives
Café hosts initiated the roundtable discussions by sharing each table’s designated prompt as well as synthesized responses from each rotating group. In doing so, attendees were encouraged to challenge or complement the café host’s summaries, although attendees had the ability to steer their conversations in whichever directions they felt drawn to. Café hosts also facilitated dialogue between attendees utilizing probes and responses to segue between points of discussion. Given each group’s diverse positionalities, their conversations were unique; however, the primary themes were enriched by additional perspectives that included the importance of acknowledging implicit bias and the well-argued role of occupational therapy practitioners to be critical advocates for services, referrals, and situated care. Preliminary findings from each prompt are as follows.
Prompt I conversations were dominated by two themes: 1) the tensions within negotiating intersectional and culturally situated understandings of health within larger structural understandings; and 2) the importance of diverse racial and disability representation and community-centered partnerships amongst occupational therapy practitioners.
Negotiating Health. Responses highlighted the tensions attendees experienced when attempting to define health and identify influences on health. Attendees noted the importance of understanding different conceptualizations, in particular, how health is defined by the lexicon of a culture but implemented or practiced in individualized ways. Culture in this sense is not limited to Black and other racially minoritized people, but includes disability as a cultural group as well. While practitioners discussed this critical distinction, they also noted that how health is understood is often determined by society at large (and subsequently by the dominant group) as well as the institution in which one is employed.
Representation and Connecting to Community. There was consensus that occupational therapy practitioners can influence health, and recognition that their influence is situated in a broader sociopolitical context that mediates how understandings of health are perpetuated, accessed, and practiced by Black people with IDD. Attendees also noted that to influence the health of Black people with IDD, occupational therapy practitioners are assumed to have access to the population, and that whatever access they do have is unproblematic. Although attendees were not specifically asked to reflect on whiteness ideologies, their candid conversation yielded an acknowledgement of its role in sustaining inaccessibility. Attendees went on to remark that disparate representation of Black people also occurs within the occupational therapy workforce and suggested that this problem, in addition to accessing the Black IDD community, might be confronted by cultivating cultural bridges and enhancing therapeutic relationships through diverse representation.
Similarly to Prompt I, two central perspectives arose from Prompt II: 1) accessing occupational possibilities and 2) leveraging power and privilege. On matters of health facilitators, both perspectives were situated under attendees’ shared belief that occupational therapy practitioners could serve as “agents of possibilities” as it pertained to positively impacting the health of Black people with IDD.
Accessing Occupational Possibilities. Occupational therapy’s agency was most prominent through the ability of practitioners to increase exposure to unexplored and inaccessible occupations. Attendees echoed the importance of dialogue with clients surrounding their occupational choices across rotations. They felt that increasing occupational possibilities required tact to ensure client-centered practice and recommended that a first step to doing so is familiarizing oneself–and community partners if they are unaware–with existing (or absent) community resources and their associated occupational demands. Although outside of the scope of occupational therapy practice, attendees recognized that occupational therapy was only able to become an “agent of possibility” when Black people with IDD received an official diagnosis and they remarked that this was one of the most significant facilitators for health.
Leveraging Power and Privilege. Expanding upon responses in Prompt I regarding negotiations of health, attendees also shared that occupational therapy practitioners should be intentionally reflexive about assuming authority around which occupations their clients should pursue. This sentiment was elaborated upon in Prompt II to not only be more cognizant of the cultural privilege and power ascribed to being a healthcare practitioner, but to strategically leverage it to facilitate better health for Black People with IDD. Attendees recognized that regardless of one’s socio-political positioning, the mere fact that they were practitioners afforded them structural power to influence the health and well-being of Black people with IDD. This recognition was accompanied by an understanding that occupational therapy practitioners have a responsibility to amplify, not assume, community perspectives not only within healthcare encounters, but across institutional and political contexts.
Given Prompt II’s orientation towards facilitators, the responses discussed above exhibited a noticeably positive tone regarding service provision. This understanding of occupational therapy became more nuanced as attendees began exploring the discipline’s relationship to barriers. Thematic dialogue central to Prompt III included: 1) intersectional preparedness to engage Black service recipients; and 2) problematizing “knowledge”/critically interrogating what is known about Black people and people with IDD.
Intersectional Preparedness. Feedback concerning barriers to health for Black people with IDD confirmed that practitioners recognized there are unspoken or unacknowledged requirements they must fulfill to meet the community’s needs. Attendees characterized these requirements as a radical confrontation of one’s social position; that is, sitting with how being racialized as white and able-bodied influenced their perceptions of and preparedness to engage Black people with IDD. Coming “into awareness” must accompany a process of unlearning and relearning that brings into focus the intersections of culture, race, and disability by recognizing as well as addressing bias, cultural differences, and privileges/power acquired through one’s racialization.
A Critical Interrogation of Knowledge. Attendees unpacked how coming to “know” the community (i.e., Black people with IDD and their care partners) you are working in as a practitioner also requires a nuanced understanding of the sociopolitical history of disability and how that history intersects with anti-Black racism. Attendees, again, identified deficits in practitioners’ understandings around disability and anti-Black racism as a structural determinant of healthcare access for Black people with IDD; and specifically, that unchecked biases and cognitive shortcuts may lead practitioners to enact care in harmful ways. General consensus among attendees was that occupational therapy practitioners, while enablers of engagement, must contend with their role in upholding old and reinforcing new restrictions to care through intentional learning, relationship-building, and advocacy.
Principle 6: Listen Together for Patterns, Insights, and Deeper Questions
Following the roundtable discussions, attendees reconvened in the large group to report out what they had discussed with the opportunity to comment upon what was being shared from other groups. More specifically, the first author facilitated a large group discussion that led to collective insights about commonly held problematic beliefs about health, health equity, and Black people with IDD, as well as identified areas for future action in occupational therapy practice. This engagement process reinforced the basic assumption of TWC that attendees, as a collective, possess the necessary knowledge and skills to confront the respective problem and, thus, are not reliant on other or outside “expert” solutions (Shiele et al., 2022).
Principle 7: Harvest and Share Collective Discoveries
The authors developed a coding structure for analysis with health, disability, social and structural determinants, and occupation categories. All definitions and categories were adapted from the existing codebook for the larger CPAR study. To establish reliability in their amended coding structure, each author reviewed the transcripts from the primary presentation and each subsequent café roundtable and discussed their application of the codes. They adapted the aforementioned codes and refined definitions to ensure clarity and consistency. TWC datasets were later triangulated by comparing and contrasting those data with the dataset from the larger CPAR study. The authors identified convergences and divergences and integrated those findings to strengthen the validity of their preliminary conclusions.
The first author shared the datasets and café hosts’ insights from TWC during a scheduled meeting with research partners with IDD and their care partners. During that meeting, research partners reflected on the thematic responses from conference session attendees, noting where there was alignment to their experiences and understandings of healthcare access and utilization for Black people with IDD (e.g., people who are multiply marginalized face greater disparities to care and as a result experience poorer health outcomes); as well as where each group’s attitudes diverged on occupational therapy practitioners’ role in uprooting barriers to accessible healthcare. This discussion demonstrated to be valuable fodder for research partners with IDD to prioritize which TWC themes were essential to address with the newly recruited provider partners in the next phase of the study.
Insights on Adapted Applications of TWC
Employing TWC methods during a conference presentation demonstrated several advantages and limitations to its use. The following insights, along with the lessons learned, are presented below.
Advantages of TWC
Applying TWC as part of a conference presentation allowed the first author to address the enduring challenge of recruiting occupational therapy providers to partner in the larger CPAR study. Their participation translated to three occupational therapy practitioners (two Black males and one white female) and two occupational therapy educators (both Black males) joining the larger research team at the level of co-researcher. Further, the participatory context facilitated feedback among two communities that are often not in conversation, Black people with IDD and providers. Interviews from Black people with IDD and their care partners informed the questions explored as part of TWC (Johnson et al., 2025); subsequently, provider responses from TWC enabled additional questions and dialogue that facilitated the merger of these groups within the larger CPAR study. Their responses at the conference themselves were generated in a context steadfastly structured around the explicit concerns and perspectives of Black people with IDD. This effectively flipped the power differential between these two communities–a differential that was itself elucidated by the findings outlined above–while also mitigating the risk and harm arising from such a differential for those who are multiply marginalized in ways that would be more challenging if both communities were meeting for the first time in a similar context.
We cannot confirm whether comments about power would have been shared with as much candor or comfort if the study’s community research partners had been present. Still, they are themselves a testament to TWC procedures being structurally flexible (Bumble & Carter, 2021). Sometimes described as an “unmethod” (Monforte et al., 2023), TWC was not static but evolving as attendees co-created space conducive to stimulating dialogue in ways most relevant to their lived experience. This co-creation organically encouraged contributions from all attendees by admiring the diverse knowledges (i.e., practitioner and student perspectives, educator expertise) they brought to the conversation as facilitated by the casual, conversational setting. This translated to an organic exploration of a variety of sensitive and controversial topics (e.g., anti-Black racism, white supremacy in healthcare) during large and small group discussions which may require more time to breach in traditional research methods.
Authors also noted the unanticipated benefits to participating in TWC. Following the roundtable discussions, attendees reported that for many of them TWC was their first experience participating in a research activity. Its structure made research more accessible to those who did not have formal training in research methods, which ultimately contributed to increased study enrollment as previously mentioned. For example, one practitioner remarked, “It was a fun way to engage in research and help practitioners see the value in what researchers do… and make a conference presentation interesting.” A student attendee added, “…it helped us see that [we] also have something to contribute as emerging practitioners. I’m still learning but have lived experience and other insights.” Attendees also reflected that allowing those at various stages of their careers to engage collaboratively increased information-sharing and opportunities to partner in professional endeavors of other peer attendees.
Limitations of TWC
Kitzie and colleagues (2020) noted methodological limitations of TWC, namely: “failing to account for power imbalances, suppressing dissent, and lacking reflexivity. These weaknesses emanate from a central claim of TWC that envisions conversation as occurring in a vacuum from the external world, where power differentials are temporarily suspended” (p. 8). This, too, was evident from observations of TWC with occupational therapy practitioners, however to a lesser extent given their shared professional positionality. When foundationally implemented, TWC procedures do not sufficiently facilitate critical reflexivity among its participants. Attendees in the study example were neither probed to interrogate their social locations nor how the sociopolitical context shaped their conversations, including the influence of the first author on their exchanges. Although there were brief mentions and reflections by attendees concerning power and identity, there was no intentional explication of how one’s positionality impacted (a) why they selected the particular session, (b) why they elected to consent to the research activity, (c) what they brought to the conversation, and (d) how their responses were informed by their lived experiences. To address this deficit, Ketzie and colleagues (2020) recommended that café hosts document who is present at each table for each round (e.g., number of participants, gender, race, employment classification) to match identities with topics of discussion and analyze how participants’ identities influence content and flow of conversation. This strategy will be implemented should we elect to use TWC again.
This also highlights the structural limitations of TWC, as a research method, in addressing power differentials in conversation. While power hierarchies in the study example were subverted between some groups (i.e., Black people with IDD and providers via the structuring of the session and who was physically present), the same cannot be said for other intersectional positions amongst providers as TWC itself does not flatten power hierarchies; rather, there may be an inadvertent reproduction of hierarchies as the discussion prompts were not developed in collaboration with conference attendees, and there was no mechanism to contest or amend prompts. We also note the inclusion of occupational therapy students as café attendees as one such example where hierarchy went intentionally unchallenged. While attendees of the study example reported feeling included and valued as contributors, student attendees in general may not feel as compelled to challenge educators and practitioners in dialogue, given the often authoritarian positions that such persons occupied during their occupational therapy training. This is not to suggest that this step could not be taken by the café hosts; but is not a prescribed component of TWC.
Lessons Learned from TWC
Although modifications to TWC protocols increased the possibility of conducting one at a conference, fidelity to or expansion of these protocols in future endeavors is highly encouraged. Reflections on the case example revealed that deviations around time constraints and documenting conversations provided notable methodological lessons to inform TWC moving forward. Regarding the timing of prompt conversations within TWC, while it could be said that shorter time intervals revealed to attendees that they had more to contribute in responses than at first glance–possibly contributing to the motivations of the five attendees who later joined the study–future work should strive to provide as much time as possible for conversations to take place. Increased time to converse allows attendees to have more time to process and share their experiences, thus enriching their responses while also supporting the integration of previously outlined opportunities for critical reflexivity, prompt contestation, and collaboration. Within a conference, this may require reorganizing the presentation to prioritize TWC; however, given the context’s structures, additional avenues are recommended to hold space for conversation.
Just as important to the conversations being had is how they are documented. Given the layout of the conference presentation (See Figure 1; i.e., all prompt discussions occurring in close proximity), despite each prompt discussion being recorded by the cafe host, the room often became too loud, or attendees were too far from a microphone to be captured. Multiple manual transcription cleanings were conducted to ensure responses were documented as verbatim as possible, but some phrases remained unintelligible in the recordings. Future endeavors could benefit from multiple recording devices dispersed across each prompt table to improve data capturing or greater distance between these tables to mitigate noise pollution within recordings. Incorporating the use of attendees’ written notes (e.g., through flip charts, tablecloths, etc.) could also help minimize documentation concerns that emerged throughout TWC case example. Providing attendees with the opportunity to document themselves, in addition to a café host, aligns with TWC protocols for increasing participation. This approach also serves as an alternative recording mechanism, which can help mitigate concerns about audio recordings. Attendee note-taking also adds an additional layer of data interpretation for the community engaged in the conversations, as it directly records their impressions of the conversation. Together, note-taking dually supports data collection while also enhancing the agency and power of attendees.
Power, however, is mobilized beyond increasing the autonomy of attendees, and our TWC reiterates the importance of managing power and structural inequalities. The limitations of TWC regarding power and potential strategies to navigate them are discussed in more detail above; however, it is necessary to highlight a specific consideration related to using the method at an occupational therapy state conference. It is essential to acknowledge that this TWC example, like most research endeavors, was contingent upon who attended the presentation. This raises methodological and analytical implications around who is represented writ large at these conferences and who is likely to attend a session related to health equity for minoritized people with IDD. For example, it was found that occupational therapy practitioners in North Carolina “fell short of matching the proportions of the State in all racial/ethnic categories” with less than 15% identifying as non-white (Lombardi et al., 2024). This does not account for additional intersectional considerations such as disability or the makeup of the conference itself. Ultimately, while conference and professional meetings have the potential to be spaces for transformative action, data collection, and recruitment, this highlights the need for more traditional and established methods for targeted recruitment of providers to participate in research.
Conclusion
TWC offers health service researchers novel strategies that allow for rapid yet conscientious data collection. Amidst ongoing calls for justice-oriented research practices, TWC methodologically seeks to generate a research context that holds the potential for participants to move from subject to co-researcher. Through collaborative and community-led conversation, data is more democratically generated and representative of individual, community, and structural experiences. Actualizing the potential of TWC, however, requires critical reflexivity on the part of hosts and attendees to best account for, critically interrogate, and flatten power hierarchies. Additionally, while TWC protocols are flexible, they are only to a point and researchers should be mindful of the potential consequences of adapting the method. Through a case example of TWC at a conference, the utilization of the method has been demonstrated to improve recruitment and retention of provider partners, support funding-dependent data collection timelines, and consolidate transdisciplinary practices.