Introduction
Throughout the entirety of this project, Community Based Participatory Research (CBPR) has remained as the required, relied upon methodology. This project was unexpectedly launched in a research design, later encompassing turns in study implementation and unexpected results. Next came the unexpected transition task from research findings into identifying a tangible solution reflective of the results. The project progressed from academia into entrepreneurship through the designing, building, testing and validating of the web platform, tools and business models; all the while creating and testing marketing strategy. Despite the different stages from research through tangible solution building and implementation, CBPR provided the specific guidelines to establish a sustainable permanent community engagement framework and collaborative decision making. Furthermore, CBPR outlined the processes that unexpectedly led to My Needs Network becoming a networking service provider for the disabled community.
Just as the study results came as a surprise, so did the emergence of My Needs Network. This manuscript provides a walkthrough of each phase of the My Needs Network lifecycle thus far; and how participatory research methods are not only relied upon, but support the transitional challenges between the different stages. The manuscript moves through eight years of research, software building, marketing strategies and business models. Throughout these years, not only does the CBPR research findings sustain as a primary focus to the overall project, but also demonstrates how the CBPR approach drives transition and building well beyond the research phase. In other words, this project in its entirety serves as the proof that a community-based and participatory research project can give rise to a community-based and participatory solution to problems identified in the research. In the case of My Needs Network, it all started with the question, ‘what does the disabled community need?’ CBPR not only allowed us to attempt to answer that question, but to build a solution to that question, sustain that solution, and create awareness of the solution.
This manuscript describes the eight-year journey of taking a call for answers to a community-based need and applying participatory research principles to first identify those answers and then, through a series of steps, transition the answers and participatory research principles into other industries and fields. This multi-industry shift was required to create a tangible, sustainable living system designed to fluidly address the community pain points. Specific to CBPR, this manuscript describes the unexpected pathways of first establishing CBPR methodology in an academic ‘comfort zone’ project and then keeping with the methodology and fundamentals to move beyond academia in order to effectively, fluidly and sustainably deliver solutions.
We first provide an overview of the initial CBPR research (Phase I), how it led to CBPR research and analysis (Phase II), and how the research results transitioned into designing and building a tangible product to meet community needs. Phase III is the creation of a Minimum Viable Product (MVP) for community review and feedback while simultaneously developing sustainable business models. Phase IV serves as the live web-based platform, its management and sustainability, and the continued commitment to CBPR and community involvement.
Phase I. Research
Background
Children with Complex Medical Conditions (CCMC) are defined as having special health care needs involving three or more systems; requiring the use of technology; and utilizing more services than the average child. Diagnoses are measured by complexity, level of functioning, and need which requires a significant amount of healthcare resulting in some of the highest utilization and financial costs in pediatrics (Carvalho et al., 2021; Sidra et al., 2022). Although CCMCs make up less than 5% of the overall child population, they account for about 50% of total Medicaid spending on children and more than 30% of all pediatric healthcare costs (Agrawal et al., 2016; Corden et al., 2023; Sidra et al., 2022).
For over 20 years the American Academy of Pediatrics has advocated for all children with life-threatening illnesses to receive access to palliative care in an integrated model (American Academy of Pediatrics, 2000). Pediatric Palliative Care’s home-centered, medical home delivery of clinical and non-clinical health services centers on a variety of holistic care methods around the patient and family (Rogers et al., 2021). To implement strategies that reduce utilization and costs for the CCMC population, a patient centered medical home needs to reflect improvements in outcomes in health-related quality of life and quality of care; and the CCMC population needs to be actively involved in all components of the strategies. This level of community involvement can lead to further ideas and opportunities for reducing healthcare costs and utilization through patient/family-centered care delivery (Community Hospice & Palliative Care, n.d.).
Objective
The objective of this study was to better understand key, culturally relevant processes, decisions, actions, and reasoning for CCMC hospital utilization; and identify opportunities for actionable change to improve CCMC quality of life as it relates to hospital utilization. In other words, we sought to learn what the CCMC community needs (clinical and non-clinical) to ultimately improve quality of life?
Conceptual Framework
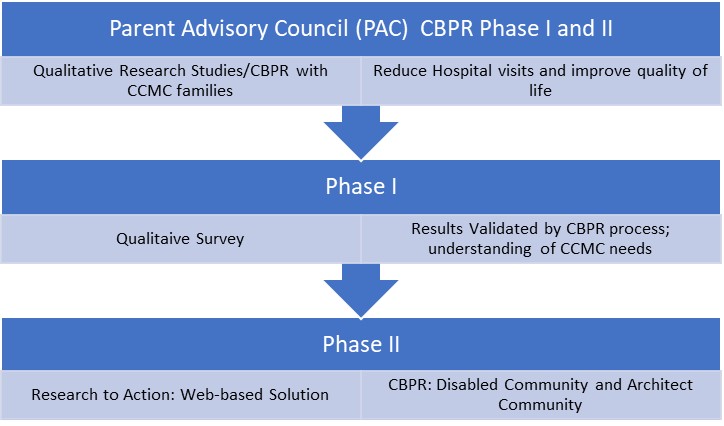
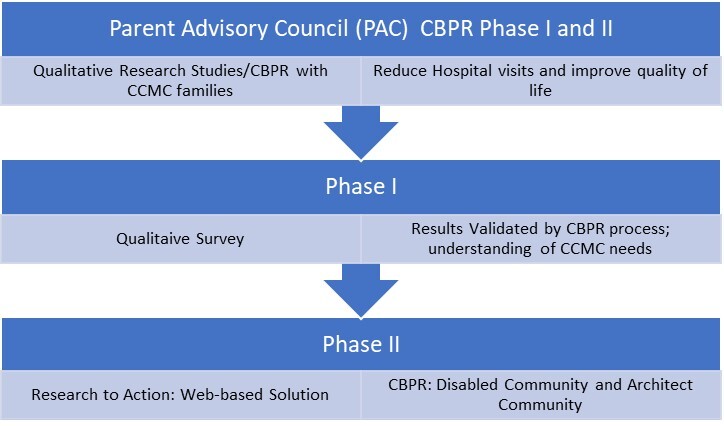
In 2014, two pediatric medical institutions participated in a three-year initiative aimed at improving the quality of care and reducing costs for CCMC. During the initiative, communication and care coordination strategies were implemented and a Parent Advisory Council (PAC) was established. Independent of but stemming from this initiative, two IRB approved qualitative research projects were implemented to learn more from CCMC families about why they utilize clinical and non-clinical services, and to better understand their ideas for ways to reduce visit frequency while maintaining quality medical care. The study design combined a Grounded Theory approach with Community-based Participatory Research (CBPR) methodologies.
CBPR provided guidance for the community’s involvement and representation throughout the entire research process. The CBPR concept of reciprocal co-learner relationship between the researcher and the researched, and the immediate and direct benefit of research findings for collective action to produce social change, were utilized. The CBPR process of group formation and functioning was used to facilitate open dialogue, generate divergent views, and develop outcomes (Amauchi et al., 2021; Vaughn & Jacquez, 2020). All the while, CBPR’s framework and emphasis was reflected in the importance of communication, community engagement, and equitable partnerships throughout the research process (Shelton et al., 2023; Vaughn & Jacquez, 2020).
The process was implemented in the following five phases:
-
Partnership formation and maintenance
-
Community assessment and diagnosis
-
Definition of the issue
-
Documentation and evaluation of the partnership process
-
Feedback, interpretation, dissemination, and application of results" (Livingood et al., 2016).
Combined GT-CBPR
A Grounded Theory approach guided both data collection and analysis, allowing social processes and community needs to emerge organically from the data (Charmaz & Thornberg, 2020; Turner & Astin, 2021), while CBPR integrated the knowledge and input of CCMC parents, families, and providers to develop strategies to change and improve community health (LoIacono Merves et al., 2015). This combined methodological approach enabled both systematic analysis and meaningful community engagement throughout the research process. Together, GT-CBPR approach provided a thorough understanding of the CCMC community’s knowledge and experience specific to the barriers and needs related to accessing resources and care. This study adopted an ethnographic perspective, that what the community voices drives the research and the analysis. As a result, CBPR is a methodology in and of itself and does not need to be bolstered to appeals to other approaches to don a veneer of scientific validity.
Data Collection
The data collection process was designed to collect qualitative data on CCMC parents’ insight to improving CCMC patient and family quality of life. This took place through (1) learning from the parents how best to collect the data; and (2) implementing the process learned in (1) to collect the data. In our case, an emailed online survey comprised of open-ended questions was used.
Data collection occurred as CBPR I and II. CBPR I was a 12 month process that took place during monthly Parent Advisory Council meetings. The primary focus of CBPR I was to develop a CBPR team and ultimately build a data collection tool and process for learning more about CCMC access and utilization of resources. CBPR II was six months and the purpose was to implement the online survey tool designed and built by the CBPR team in CBPR I to collect data from the larger CCMC parent population.
CBPR I
During CBPR I, a CBPR team was established; and the subject areas and methods were defined for data collection. The CBPR team included the Community Team (parents of CCMC), the Internal Team (comprised of a principal investigator, two research manager investigators, and a parent liaison), and the Provider Team (faculty and staff of the academic center and community hospital).
The Community Team’s role was to serve as the population experts and advise the Internal Team on ways to best connect with and learn from the broader population of CCMC families. The Internal Team applied research practices and CBPR methodology in facilitating the Community Team meetings and discussions. This involved taking the Community Team ideas and suggestions and implementing them as actionable research by applying CBPR principles, qualitative research applications, and institutional research requirements. The Provider Team provided additional input and opinion on the study design, data analysis, and results.
CBPR I-Data Collection
The initial data collected was related to CBPR team formation, merging community team content and direction with CBPR research methods and concepts, and content related to the open forum discussions with the community team. This included content gathered from CBPR team meetings and discussions related to the various clinical and non-clinical services utilized and needed; and how these services can be improved. During the team meetings, the following two questions served as the initial central focus point of the conversations:
-
What do we need to learn related to receiving care, accessing services?
-
What do we need to learn to address problem or issues related to receiving care?
The feedback led to developing additional questions (See Addendum) discussed by which were reviewed by the Provider Team and then presented as a group activity during the community team member meetings. Answers were reviewed by the Community and Internal Team members and used to design a web-based survey. Although the Internal Team proposed focus groups, the Community Team determined an online survey would be the best option.
During CBPR-I, the focus was on survey design and development, survey question builds, developing survey invitation letters, and designing survey delivery methods. The final data collection tool was a web-based survey, comprised of nine sections and a combined 56 open ended questions. The survey distribution design was a monthly email to approximately 400 parents of patients of the clinics providing care to CCMC. The goal was to collect responses from 100 of the 400 parents emailed. Upon the completion of each survey, participants were invited to join Parent Advisory Council meetings and learn more about the overall project.
CBPR II – Survey Distribution
CBPR II consisted of the CBPR I survey distribution, data collection and analysis. The following table provides an overview of the specific components of CBPR I and II:
Analysis
Grounded Theory was the systematic analysis approach in order to capture the theory that emerged. The Grounded Theory process incorporated Open, Axial and Selective coding to find relationships, identify common themes and ultimately build three tiers of categories. The survey closed with 745 responses and an overall 70% response rate, based upon the goal to receive 100 completed surveys. Because the survey was designed as nine primary questions with 56 sub-questions, a data dictionary was developed to identify a subject area that each question and response was grouped. Next, the data set was restructured by moving each response from the original sub and primary question to the categories, subcategories, and underlying themes that had emerged from the responses. Prior to moving data, each individual response was coded by Category Color Code, Question Number, Sub-Question and Subject Area
To better identify the level of importance of a category or theme associated with a particular question, as well as the depth of response measured by the amount of content provided, the Internal Team designed a system to better comprehend the effort put into each response. It is important to note that the ‘weight’ or breadth of the response was a key factor in the analysis and provided valuable feedback. This is especially important due to (1) the general cultural nature of CCMC parental responsibilities, stressors and hardships; (2) while also being very constrained for time due to the multiple challenges associated with caring for their CCMC; and (3) taking the time to complete a survey comprised of 56 open ended questions with no participation incentive. Because the completed surveys resulted in such in depth responses, the Internal Team deemed it important to account for the time and thought a survey participant put into a response. To objectively measure the time and thought put into the responses, the Internal team created a system to weigh responses by the amount of content. For example, the average response for all 745 responses was a 2.6; indicating that most participants’ responses ranged from a complete sentence to a complete sentence combined with a sentence fragment. This weighted response system further allowed the Internal Team additional information in the process of identifying themes and categorical areas of importance. Below are the average weighted scores of total responses of the highest weighted categories; which led to identifying our final categorical areas of need:
The second phase of analysis consisted of reviewing the data analysis notes for each of the 745 responses; summarizing recurring commonalities, themes, interests, concerns; and reviewing weighted values, reoccurring words and phrases, and the Internal Team members’ notes. The analysis process provided a collective, final review and interpretation of each survey response, and a way for identifying categories, subcategories, underlying themes, level of value or importance to the population, and key words/phrases. As a result, the following eight categories were identified as the most representative of the survey responses: 1) Suggestions and Barriers, 2) Legal, 3) Financial, 4) Transportation, 5) Services, 6) Expenses and Supplies, 7) Training, 8) Communication.
The final phase involved the Internal Team going through each category, reviewing each response, investigator and team notes, and reasons responses were transferred to a category. This exercise allowed the team to test the category to ensure the data assigned belonged; re-define the category if necessary; and identify examples of survey responses that best represented the category.
Results
The results of the qualitative data analysis reduced the total number of categories from eight to four, identified subcategories, and sub-subcategories. The following table provides an overview of the categories that emerged:
Several reoccurring themes emerged throughout the subject areas, category, subcategory, survey questions, and weighted responses. Themes emerged through a multi-phase analysis process where team members first evaluated individual responses using the weighted scale and provided detailed notes including their perspective, summary, and categorization rationale for each response. Subsequently, these 745 responses were systematically analyzed by reviewing recurring patterns, weighted values, and team notes, while using color coding to track response origins and maintain counts of responses within emerging categories. This methodical process culminated in the identification of seven main categories that best represented the survey responses. The common themes included: timeliness, emergency room aversion, feasibility, community networking, and resource awareness. The following table provides an overview of the emerged themes:
Phase II-Transitioning from Research Results to Product Ideation: Design and Development
Background
Immediately following the completion of the two-part qualitative study, the supportive funding ended and put a close to the overall project. At this point two questions had to be answered as to what to do next: Do we continue academically and immediately focus on publishing and presenting the research findings as an investigator initiated study? Or do we step outside of our academic role, independently finance, and move into the unknown worlds required to try to build exactly what the community is asking for? Without funding or additional staffing support, the latter was chosen as the next step. As a result, and over the course of two years, the project took on multiple stages and roles in entrepreneurial ideation, web design and development, feasibility, and validation.
Objective
The objective was to build a tangible representation of what the community was asking for in the research findings’ identified categories, subcategories and underlying themes. At the onset of the design phase, it was unclear what the end product was going to be, except that it had to be a clear reflection of a free, easy to use system that community members could access. It needed multiple categories identified as ‘high demand’ resources and also needed to contain various networking functions that create awareness of the resources available and how to obtain them.
Design and Development
To achieve the objective, the research findings slowly transitioned through stages of product ideation, platform model development, strategic planning, validation, and eventually the build of a tangible resource. To remain in line with the community’s requirements the following rules were applied:
-
‘Community’ is defined as any individual with a disability, their family members and care takers, social workers, case managers, physician; and any clinical or non-clinical institution, program, company, organization, or individual who provides for or works with individuals with disabilities.
-
The tangible item to be developed needed to be free to the entire community.
-
To be available nationwide.
-
A ‘Community ownership’ concept.
To ensure the design and build remained a true reflection of the community, the five CBPR Phases continued to be implemented:
-
Partnership formation and maintenance
-
Community assessment and diagnosis
-
Definition of the issue
-
Documentation and evaluation of the partnership process
-
Feedback, interpretation, dissemination, and application of results. (Livingood et al., 2016).
Following several months of additional conversations, interviews, scheduled calls and meetings with parents, care providers, tech start up entrepreneurs, and web application developers, it was determined that a web platform concept would be the first step toward a realistic and feasible solution to a tangible reflection of the study findings.
Applied Participatory Methods
Partnership formation and maintenance
Phase II initiated the most challenging interdisciplinary transition experienced to date. To implement this phase and continue participatory practices and community assessment of the project, the community partnerships were divided into two sectors: (1) Disabled Community: Social workers, case managers, pediatricians, health administrators, and parents; and (2) Architect Community: entrepreneurs, platform developers, web developers, and web designers. Both groups were engaged with at least twice a week for approximately one year.
Community assessment and diagnosis
Because the ‘community’ had expanded into two separate arms- Disabled Community and Architect Community, the CBPR Community Assessment and Diagnosis phase became more of a connector piece that started to bridge ideas, needs, and values into realistic, feasible design outcomes. For example, the Disabled Community members would review plans, builds and next steps; and determine if those next steps will serve as an overall solution to the parents and families. This would allow for additional tweaks and builds to adjust to the Disabled Community members’ suggested edits and most importantly the needs and solutions that can be addressed via a web platform. Feedback would be taken down in meeting minutes or notes and then applied to the actual design and build.
Definition of the Issue
The ‘issue’ being the need for a tangible build slowly began to take shape, evolving while remaining stable to the core community’s needs. For example, the Architect Community would receive the Disabled Community team’s feedback and updates and determine how best to integrate the changes into business models and strategy and the web-based product. Occasional challenges would arise when a design or concept would be considered too difficult typically based on navigation, utilization, or potential cost in time or money for the Disabled Community. The idea would be modified and discussed with the Disabled Community Team for review and evaluation. As a result, the definition of the ‘issue’ transitioned from a need for a tangible tool, reflective of the community needs, into being the ‘tangible tool’ as a community driven web platform. In other words, the concept of a web platform was thought to best represent the needs related to the community’s voice related to a tangible tool that is easy to use with the ability to learn and connect with other community members in effort to increase awareness and access to resources.
This transformation meant that the web platform would serve as an interactive repository for community networking centered around providing information about both specific types and generalized categories of resources, information, services and tools.
Documentation and evaluation of the partnership process
The primary focus of the design and development phase was the actual, tangible build of a web platform that emphasized a process that relied upon both communities’ participation. Feedback was in the form of verbal or written edits and suggestions, ideas and requests; and received from both the Disabled and Architect communities through meetings, emails, and phone calls. For example, when discussing and interviewing social workers or case managers, their feedback would primarily be focused on the types of resource categories to be displayed. When asked about ‘what they need in a special needs website or platform’ their feedback was for tools or opportunities within a platform that would save them time in resource searches and connecting patients/families with the resources. This information was then brought to the Architect Community where the web design and developers provided potential ideas for addressing this feedback while keeping in mind the ease of use for the individuals and family members and the responsibilities and tasks for the case manager and social workers.
Design and building of the business model was also a focus during this phase. From an entrepreneurship point of view, the justification for the tangible build without a tested business model is normally not encouraged, however, because the research data findings were so clear in determining the need for the tangible build, justification for financing the build of a minimum viable product alongside the business model build was acceptable. Moreover, in this particular situation of building a product that is to be free of charge for all end users, and designed in such a way that the community drives both content and the types of tools and resources that make up the platform, the idea appeared too grandiose and widespread for an effective business model without the tangible product alongside. Lastly, we decided not to delay the tangible build despite the business model not being clearly defined.
Throughout this phase of the journey, there were several instances of Disabled Community representatives referencing other tools, websites, or platforms with similar initiatives that were unsuccessful or no longer active for reasons such as difficulty of use, insufficient number of users, cost-based for the end user, client only access or inability to access, or project funding ended. This feedback proved to be extremely beneficial as the project has grown and evolved.
Upon finalizing development of a minimally viable product, the real challenges were related to overall solutions for sustainability, and for potential investors. In other words, at this point in the overall project (Phase I Research and Phase II Development) we had identified: (1) a clear problem: there is not a single tool, easy to use, free of charge, designed specifically for the disabled community to connect and network with a variety of disabled community members in searching for and obtaining a need; and (2) a clear solution which is to create a tool solely designed to solve the problem. However, we were beginning to understand why a community-driven platform had its challenges: because of the difficulties associated with an effective business model to provide a pathway to overall project sustainability.
Phase III- Minimum Viable Product, Business Model and Validation
Objective
Following the design and build of the minimum viable product, and the initial business model builds, Phase III was initiated. This was a two-year validation stage comprised of presentations, demonstrations, edits, validation, and adjustments to both the minimum viable product and business model. During Phase III, participatory research was adjusted to include the web platform and business model participants. Partnership formation grew beyond the current communities to include organizational partnerships, marketing experts, and additional software and business model experts. Challenges remained with addressing the community’s need for a free and easy-to-use web-based platform and had to align with a sustainable design and a developing business model that would not implement revenue sources from any part of the disability community.
As the platform and models developed, there was a slight shift in community focus from parents and family to social workers and provider. Assessment became more focused on the provider needs in a platform; and whether the platform designs were solutions to those needs. In other words, begin using My Needs Network to assist and support the expert service providers within the disabled community. For the provider, the definition of the issue was adjusted to questions of sustainability, database upkeep, and best practices for documentation and database management. Already having the minimum viable product allowed for more efficient Disability Community involvement in that the ‘idea’ could now be demonstrated rather than explained as a concept. On at least a monthly basis, MVP demonstrations were held for Disability Community provider organizations; consisting of a brief slide deck presentation and a walk-through of the platform.
Business Model
During the MVP Phase III, the business model did not involve the Disabled Community, however participatory research method findings from the Disabled Community continued to be applied to the overall project. The participatory research focus for the business model became the Business Community members. These members included various entrepreneurs, entrepreneurship training program leads, and business model mentors. The issue quickly became the question of sustainability- how a web platform could not only be built but also sustained for a vulnerable community inclusive of individuals and organizations with limited budgets. The business model had an unclear revenue source. The Business Community members generated ideas and business models which the group then tested and validated, with feedback provided throughout the process. Documentation was collected in tools such as the Business Model Canvas, which generated suggestions and feedback documented in business model drafts (Business Model Canvas, 2023).
I-Corps
My Needs Network (as a minimum viable product) also participated in the U.S. National Science Foundation’s Innovation Corps (I-Corps™) program (NSF’s Innovation Corps, 2024). I-Corps is an entrepreneurial training program that facilitates the transformation of invention to impact. Designed to prepare scientists and engineers to extend their focus beyond the university laboratory and accelerate the economic opportunities with early stage projects, the I-Corps program allowed for further engagement and mergence between the Disabled and Business Communities. Through a customer discovery method of identifying the potential end users and decision makers, and their true needs in relation to one’s product, a second type of qualitative data and participatory research was implemented; this time from the business model perspective.
The I-Corps program provided My Needs Network an entrepreneur mentorship partnership who would facilitate and guide qualitative, customer discovery data from various nonprofit organizations, companies, rehabilitation facilities, and medical supply providers. Assessment of these organizations’ true needs around networking and access to resources for either themselves or their clients became the primary focus. Documentation and evaluation were completed through the I-Corp’s program format of individual and group meetings, project updates, and documented using I-Corps customer discovery templates. Feedback was derived first from the interviews and then through the trainings and mentorship. I-Corps aligned with CBPR in that direct engagement with potential stakeholders was implemented; and learning took place from real-world interactions and experiences to understand needs and perspectives of target populations.
Results
My Needs Network’s Phase III introduced a variety of participatory methods, which extended beyond the original focus of the disability community members and providers to include entrepreneurship, innovation and business model development, and web application and platform experts. Combined, these three communities formed a revised community participatory approach that required each of the three communities to create a single My Needs Network community. As a result, the partnership formation, assessment, redefining areas of focus, feedback and interpretation of results began to take shape of a tangible, sustainable tool that supports the Phase I research findings.
Phase IV- Platform Management and Sustainability
Overview
Over the past two years, My Needs Network has moved into its current, ongoing phase of build, test, evaluate, rebuild, test, and reevaluate. Within the current phase, the platform is live while continuing to implement the rebuilds, strategic planning, and marketing. Formative and summative evaluations are the newest areas being added to the overall project. To date, My Needs Network has taken the shape of both the tangible platform as well as a concept; all of which reflect the CBPR previously approaches discussed in this manuscript. The live project has allowed for a University co-ownership agreement, multiple organizational and corporate partnerships and collaborations, conference presentations, grant applications, robust marketing strategies, external board memberships, white label builds, end user utilization and additional tools to be built onto the platform.
Strategic planning
Strategic planning includes a variety of tasks and objectives to ensure the My Needs Network is sustainable in terms of a platform and overall purpose. Partnerships increased in all sectors including disability community members for continued platform needs, edits, utilization and evaluation; collaborations with individuals and organizations for entrepreneurship and sustainability purposes, and companies geared toward marketing, technological and product developments.
Each of these types of partnerships (community, entrepreneurial and technological) bring suggestions and modifications that were shared and merged with the other two. For example, if a new software was being considered to better automate database management, the reasoning and functioning of the software were shared with members of the disability community members who would then provide additional feedback and whether it was a ‘want or a need’. Another example is the ‘white label’ service My Needs Network provides for various communities, organizations, and events. This means that the framework of My Needs Network could be applied to solve other issues such as the needs of immigrants and refugees, homeless, or maternal and child health. This could generate revenue from the software as a service which could be used to fund the My Needs Network disability-centered platform. This concept overlaps with the technological and development spectrums of the platform and opens additional ideas and tools that can then be applied to the My Needs Network platform. These ideas and tools are then shared with various members of the disability community to evaluate their importance and value of their function.
Assessment from each of the community sectors are reviewed, and when necessary applied to either the build or the strategic plan. For example, the community specific focus continued to take place within meeting, conference and platform demo feedback; entrepreneurship feedback was mostly in the form of business model customer discovery continuation, and mentorship assessment of the platform’s current status; and technical and product assessment was through review of the capability and feasibility associated with builds and edits based on the feedback received from the community specific needs and entrepreneurship requirements. In each example, the implementation of a need or idea that was generated from one type of partnership would blend and impact both strategic planning and CBPR methodology in the other areas of the partnerships.
Marketing strategy
Marketing strategy has been the most recent area of focus for the My Needs Network overall initiative. This includes a variety of efforts to bring people to the platform and serve as a call for partnerships with the platform. The marketing strategy is two part; first is a variety of approaches to gain end user traction from family members and individuals, and the second is a partnership approach with organizations to expand My Needs Network. This second approach increases the My Needs Network brand while allowing for an unrelated revenue stream through the white label marketing that can be allocated to My Needs Network.
Marketing Partnership includes a collaboration with marketing consultant teams familiar with nonprofits, underserved communities and the disabled community. Collectively we work toward creating awareness and building connections with organizations representing vulnerable populations in providing a platform template specific to their needs. Assessment of community needs and problems are collected through a recently launched customer discovery/qualitative data collection question sets distributed to over five thousand individuals and organizations’ email and social media posts. This campaign works to not only create a marketing awareness but also collect customer feedback on the different tools, concepts, wants and needs.
Discussion
Throughout the overall initiative, from the idea for a research project to web platform development, marketing and partnership, CBPR principles and methodology were applied and served as a guide at every stage. As a result, at each stage community-driven solutions emerged and guided the project through to the next stage. Moreover, not only were each of the five phases of CBPR[1] achieved in the overall initiative; but each phase was applied and provided guidance and infrastructure to each step in developing to even marketing My Needs Network. This includes but not limited to: ideation design and development, tangible platform build, testing, business model build and validation, evaluation, marketing, and beta testing.
During the research phases of the project, while the CBPR Team developed the survey, the Internal Team communicated their thoughts and methodology-related guidance on the concept of a survey consisting of 56 open ended questions and how this may not be the best designed survey; especially given the target population and their limited amount of free time. However, the Community Team members remained firm on the design of the survey and the questions. As a result, the survey resulted in a 70% response rate (based on the goal of receiving 100 completed surveys) with 745 total detailed responses. This is important when considering the average online survey response rate is approximately 44.1% (Wu et al., 2022) which when combined with there being 56 open-ended questions, indicates that not only was CBPR effective but also identified a clear underlying theme of survey participants finding the value of this opportunity to address their opinions and feedback.
In addition to the high survey response rate, another unexpected result was the depth provided in the open-ended responses. Despite the risk of survey fatigue, the survey size and design of this particular survey, combined with the time restraints associated with survey participants, it was surprising to find the length and detail of responses throughout the entire survey. The detailed responses led to the identification of multiple themes, categories, subcategories and sub-subcategories related to their needs and requirements for improved quality of care and reflective of the target population’s needs, wants, suggestions, complaints, compliments, and reasoning.
CBPR not only allowed for parents and resource providers to have a voice in the research study design and implementation but provided the insight required for a very high response rate and detailed answers provided the CBPR team with an additional view into the need for change related to the study’s subject area. When ‘closing the loop’ in the CBPR phases, the combined results led to look for a “strategy for changes to improve community health” (LoIacono Merves et al., 2015). The strategy became the design, development, build, and model validation of My Needs Network: a web platform reflective of the findings. Moreover, My Needs Network’s sustainability model is integrated with CBPR methodology as a way to ensure the platform is consistently reflective of the community’s needs and values.
The end of the research phase marked the beginning of multiple, multifaceted phases over several years. Within each phase of My Needs Network the CBPR concepts and the research findings and underlying themes were forced to resurface to provide the needed guidance. Furthermore, My Needs Network continues on pathways of growing in areas of CBPR related community-academic partnership drivers, such as the Commitment to Collective Empowerment and Structural Governance as the fluidity of the project allows for a wide variety of community engagement and leading towards multifaceted areas of focus in benefits to the disabled community (Oetzel et al., 2022).
For example, My Needs Network’s current phase has produced 1) partnerships with community stakeholders; 2) specific tools available for the CCMC community to provide documented assessments and feedback; 3) designs to continuously reflect the community values and needs; 4) designs to monitor, evaluate, track and document activity with partnerships, stakeholders, and community members; 5) easy access for the community to provide input, ideas, and suggestions for the platform. Specific to these five CBPR research phases, four of the five CBPR phases were equally applied in the combined CBPR I and II research, transitioning the research into a tangible idea, designing and building the idea, testing and evaluating the idea and business model, testing and rebuilding the live My Needs Network, and developing a marketing strategy. The web platform itself serves as the fifth phase, however the sustainability of the platform implements all CBPR phases.
In terms of the My Needs Network partnership structure, My Needs Network implements CBPR Partnership Sustainability’s three key dimensions: 1) sustaining the relationships and commitments among partners that span from parents from the initial phase of the research, various community members and nonprofits and companies who have contributed significantly to My Needs Network growth and development; 2) sustaining the collective knowledge, capacity, and values through maintaining early identified themes, concepts and categories; and 3) sustaining the partnership funding, staff, programs, and related policy changes through the implementation of multiple business models combined with various institutional relationships and collaborations (Chandanabhumma et al., 2023). Collectively, the CBPR Partnership Sustainability dimensions have allowed My Needs Network to grow through establishing strong partnerships, through addressing each organizations areas of need and/or focus.
Currently, the My Needs Network is focused on creating awareness of not only the tools and concepts that define it, but the awareness of the networking service provider concept that is driven by the true experts within the disabled community. For example, the My Needs Network newsletters and social media posts primarily highlight resources and service providers within the disabled community. Marketing campaigns are used to create awareness that My Needs Network is here to help individuals search for resources, and assist organizations with marketing, connecting with other organizations, and also finding resources for their clients. These marketing campaigns are driven by a marketing team made up of public health researchers, organizational partnerships, an external marketing team, and parents and families of individuals with disabilities.
Limitations
During CBPR I and II research, the primary study limitation was the frequent turnover among Community Team members, due to the demanding roles and responsibilities of CCMC parents. This resulted in using meeting time to update newly consented members with general information on the research methods, the project overview, the parent’s role in the study, and current status in the study. The expectation of a consistent or semi-consistent Community Team, given the CCMC parents’ personal roles and responsibilities, was unrealistic. Future research may consider a study that fully implements a virtual or webinar setting, which may prove more feasible for the population.
Children with Complex Medical Conditions were not included in the research studies primarily due to the severity of complex disabilities within our population of focus. In addition, the children with medical complexities were not the primary focus of the study since children are typically not the decision makers in searching for and accessing services and resources. Future studies may want to consider designing a CBPR Grounded Theory framework around children’s insights and perceptions of the resources and services they access.
Within each phase following the research, there have been multiple challenges in builds, concepts, and designs, however we were able to find solutions to the majority of these challenges with limited resources and funding. Some of these challenges include the My Needs Network concept itself in the need to remain broad as a service provider and the inability to steer away from serving on a broad spectrum. This inability to hone in on specific areas of care or populations has been challenging in formulating marketing and branding. Program evaluation can become very challenging in terms of measuring the effectiveness of these broad efforts.
Business models and sustainability also create limitations. Because My Needs Network is a free tool available to both families and resource providers, some of the more subscription, fee for service or referral-based models cannot be used. Moreover, because My Needs Network refuses to generate revenue from the community which it serves, we have explored other options outside of the disabled community to generate revenue that can be then be allocated to My Needs Network. Staffing My Needs Network is also challenging. Through various partnerships and degrees of partnership; combined with various strategies in business models and platform developments, My Needs Network has been able to adapt and in fact learn and grow from these limitations resulting in a variety of alternative, cost effective solutions, and ways around the high costs associated with sustainability.
As indicated, every phase of the project required sufficient time periods to complete (each phase required two years). Some of the reasons for these timeframes were due to the continuous CBPR approach combined with sustainability. For instance, the actual research phase required two parts that both incorporated participatory research; The My Needs Network building phases implemented a CBPR approach to to multiple non-research related initiatives across multiple disciplines.
Conclusion
This study started with the following question: “What are the clinical and non-clinical needs within the special needs community?” This community-designed research project provided the answers to that question and My Needs Network delivers the solutions and aims to reduce burdens associated with the underlying themes and findings related to the ‘needs’.
My Needs Network is and always will be a work in progress. It will always be a fluid site, with a multi-faceted utilization of CBPR in every aspect of builds, operations, and agendas. At the start of the initial research question, there was no envisioning of where the original qualitative study would eventually lead, and that it would amount to anything more than a completed investigator initiated study. However, the level of value and interest that emerged from the research project was the clear indication that something had to take place beyond the traditional academic sequence of a research project.
CBPR allowed for and exposed a level of need and education from the disabled community’s perspective on how to improve care and quality of life; and what services and resources are needed. Next, the CBPR approach allowed for the population to design and be a part of the entire research process, and establish a foundation implementing actions geared toward community-based process change, but also a significant role in a multifaced platform and concept that they drive and ‘own’. By first applying a CBPR approach to the research required to identify problem and solution, and then recycling and transitioning CBPR methods outside of research allowed for realistic, fluid and sustainable reflection of a community’s requests of need in a tangible product; in this case a networking service provider. Throughout the entirety of this project, CBPR has and continues to provide the guiding principles required to continue building and sustaining My Needs Network, while addressing the current and consistent areas of need, specific to the population of focus.
Acknowledgements
The authors would like to thank Jeff Goldhagen, MD, MPH for his expertise, guidance and support during the research phase and throughout each of the stages that followed in the building and development of My Needs Network. In addition, the authors would like to recognize Ronald Lukens-Bull, PhD; Tom Ross; William Livingood, PhD; Tina Bottini and Alex Parker, PhD; and Jolene Cartagenova for their efforts related to My Needs Network and this manuscript.
The five phases of CBPR include 1) partnership formation and maintenance; 2) community assessment and diagnosis; 3) definition of the issue; 4) documentation and evaluation of the partnership process; and 5) feedback, interpretation, dissemination, and application of results" (Livingood et al., 2016).