This paper discusses the potential value of articulating two different participatory research and community engagement approaches -The Community Dialogue Approach (CDA) and Participatory Video (PV), in the context of an ongoing research project and intervention. We ask how articulation can help amplify the potential and mitigate the challenges of each approach in isolation. We demonstrate that articulating CDA and PV in an interdisciplinary project means enabling the two approaches to complement each other in ways not previously considered, and to respond to issues around scale and sustainability.
We take the concept of ‘articulation’ from cultural studies, and point, in particular, to Stuart Hall’s work. Hall defines ‘articulation’ as a form of connection that can make a unity of two distinct elements, under certain conditions. As Procter puts it: ‘Articulation, as a theoretical practice in Hall’s writing, involves linking two or more different theoretical frameworks in order to move beyond the limits of either framework on its own’. Crucially, however, and as is central to the research design of this paper, ‘this process of linkage can never be fixed or final. Articulations can only be made under a specific set of circumstances, at a particular historical conjuncture’ (Procter, 2004). Or as Grossberg suggests ‘It is a linkage which is not necessary, determined, absolute and essential for all time. You have to ask, under what circumstances can a connection be forged or made?’ (Featherstone, 2011). For Hall, articulations are always situated and contingent (Clarke, 2015), and are always the product of engagement with a particular socio-cultural context: ‘No articulation – whether the combination of social instances in a social formation or a discursive alignment of meanings and politics – [comes] with a ‘lifetime guarantee’’(Clarke, 2015). This need to balance the methodological, and ultimately transferrable potential of articulating PV and CDA must always be balanced with the site-specific insights to emerge from a specific intervention.
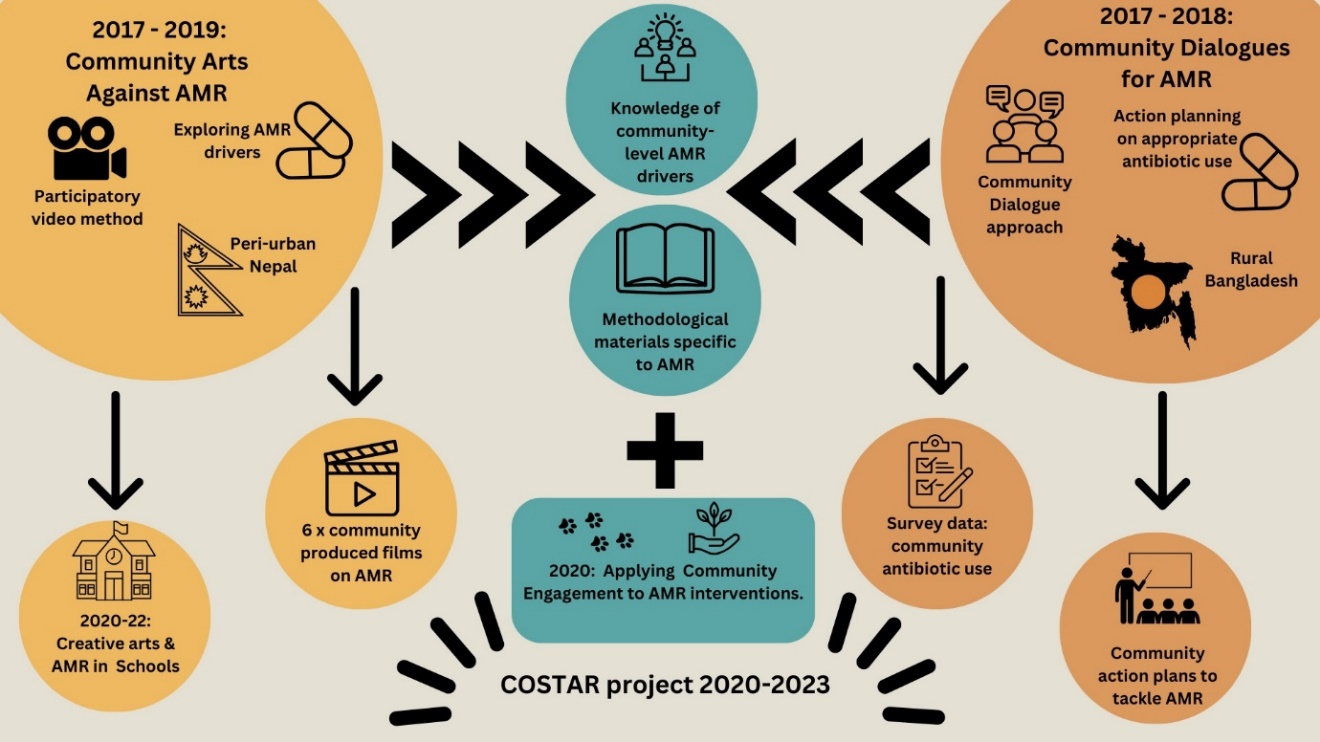
Our intention to explore articulation has developed organically over the past five years. During this time the authorship team’s network, Community Engagement for Antimicrobial Resistance (CE4AMR), has adapted, implemented, and evaluated a number of Community Engagement (CE) approaches within interventions to address the topic of antimicrobial resistance (AMR) in low resource settings (Figure 1). The network utilises a formal definition of Community Engagement agreed by all its members and co-producers to maintain consistency within its approaches:
Community Engagement is a participatory process through which equitable partnerships are developed with community stakeholders, who are enabled to identify, develop and implement community-led sustainable solutions using existing or available resources to issues that are of concern to them and to the wider global community. (King et al., 2020).
The wider literature generally holds a consensus that Participatory Research covers a wide range of different concepts including community-based participatory-research (CBPR), participatory action research (PAR), and community engagement - where collaboration is established between researchers and communities (Ormel et al., 2020). Community participation has been acknowledged as a major component of people-centered health systems and research focused on them (Cai et al., 2022). In this paper we use the term Community Engagement to refer to a form of Participatory Research that has been developed by the academic team working at the CE4AMR network, designed to both unlock community-level, site-specific knowledge about the drivers of AMR, and to support communities to use this knowledge to mitigate the impact of AMR through behaviour change and communication with key policy stakeholders.
Much of the CE4AMR portfolio is based on two well-established participatory approaches: Participatory Video (PV) (Cooke et al., 2020; Lunch & Lunch, 2006) and the Community Dialogue Approach (CDA) (King et al., 2020; Smith & Smith, 2018). There are a huge number of participatory approaches currently being used in a variety of public-health contexts, with arts-based practices, such as PV, being particularly visible (Gillibrand et al., 2023)
It is notable, however, that there is little comparative exploration of the particular value of a particular approach, or of how such approaches can be used in concert and what is achieved if they are. It is within this context that we wish to situate our work. We do not claim that bringing PV and CDA together is necessarily more valuable than bringing together any other two approaches. However, we do hope to show that working with these approaches (in which the authorship team have particular expertise) is a useful example of how to evaluate the potential of other similar approaches to ‘articulation’.
The COSTAR project (COmmunity Solutions To Antimicrobial Resistance) is funded by the UK Research and Innovation’s Medical Research Council (MRC) with a delivery phase from January 2021 to June 2024. COSTAR aims to co-develop and evaluate innovative community-led interventions to tackle the One Health challenge of Antimicrobial Resistance (AMR) in Nepal and Bangladesh and is heavily influenced by the CE4AMR team’s previous work with Community Dialogue Approach (CDA) and Participatory Video (PV) methods. (Figure 1)

Participatory video methodologies have been used in different academic disciplines to build agency, address difference across communities and achieve political impact and change (Mistry & Shaw, 2021). Many practitioner-researchers use PV in order to surface overlooked and hidden perspectives, and to build new relationships between marginalized communities and external agencies (Shaw, 2015). Recently, PV has been increasingly used as a research tool in development contexts to support communities to raise awareness of issues they face and that might not be represented in mainstream media. One area of growing interest in this regard is public health (Chávez et al., 2004; Cooke et al., 2020; Moletsane et al., 2009). However, beyond the CE4AMR context, PV has not, to date and out of the CE4AMR network, been used to address AMR, which is currently considered to be one of the biggest public health issues we face globally (Cooke et al., 2020).
Within CE4AMR projects PV has been used as an intensive intervention, taking place over short timespans (5-10 days) during which a small number of community members are supported to identify and reflect on local issues, then direct and film their own narratives around a problem they perceive as relevant (Lunch & Lunch, 2006). The final films are co-produced between participants and researchers, then ‘showcased’ to wider community members to share local knowledge on the focal issue. In some settings, these films are also showcased to policy makers as advocacy tools, as a means for communities to ‘speak truth to power’ (Cooke et al., 2020; Varghese et al., 2020).
The Community Dialogue Approach (CDA) is a longer process, typically lasting a year or more and is inspired by Paulo Freire’s transformative theory where dialogue provides opportunities for critical thinking, questioning beliefs and assumptions, and development of new ideas (Zulu et al., 2022). CDA is based on the Integrated Model of Communication for Social Change (IMCFSC) where an iterative process of community dialogue and collective action work together to produce social change in a community that improves the health and welfare of all of its members (Malaria Consortium).
CDA more broadly sits within the methodological framework of participatory methods aimed to achieve social transformation that use the articulation of awareness raising and commitment to action, for instance in research addressing issues related to reproductive health, early pregnancy and sexual health education in Namibia (Zulu et al., 2022). CDA has been used in developmental contexts such as Tanzania to address child protection as a form of participatory research and program development strategy through which developmental scientists and local community partners work collaboratively to discuss, address, and evaluate local issues in their communities (Abubakar et al., 2018).
The CDA draws stakeholders across a community to exchange ideas in locally facilitated sessions to share experiences, express perspectives, clarify viewpoints, and develop solutions to specified problems (King et al., 2020; Smith, 2018). Stakeholders are engaged in all aspects of project design, including the embeddedness of the approach into existing systems, content of materials and selection of facilitators (King et al., 2020).
CDA and PV are two distinctive participatory approaches and provide different types of engagement for community members and other stakeholders involved within each phase of the project. However, they both focus on the formation of equitable partnerships and exchanges of knowledge between different stakeholders including communities, research teams and policy makers. As such authors have become increasingly interested in the potential to combine both approaches into a single intervention.
In this paper we use the term intervention to refer to research processes and approaches used in the field of health sciences in line with the International Classification of Health Interventions (ICHI), “a health intervention is an act performed for, with or on behalf of a person or population whose purpose is to assess, improve, maintain, promote or modify health, functioning or health conditions” (Cambon et al., 2019). From an interdisciplinary viewpoint, CDA and PV can be considered as interventions as well as participatory research approaches, depending on the language and terminology used in different disciplines which is one of the themes that will be discussed later in this paper.
In addition to research outputs, the CE4AMR network also considers the challenges of CE in terms of sustainability, scalability, and the equitable exchange of knowledge between different stakeholders (researchers, community members, local gatekeepers, funders etc.). As the network has expanded, research projects have begun to utilise more than one CE approach and the focal project for this publication deliberately combines CDA with PV. We are increasingly interested to understand how such an articulation can influence both the research outputs and impacts of a project, but also the ability to scale and sustain interventions.
Within the wider literature, some authors (Zamboni et al., 2019) argue that there has been recent discussion on the different ways scalability can be understood. We consider it as a concept that requires ongoing exploration and can be understood differently in different contexts. Indeed, in practice scalability is often confused with the ability to widen the reach of an intervention, without much attention to continued robust performance under routine conditions, or to the extent to which it is embedded in a local delivery system (Zamboni et al., 2019). Scalability can then be used to emphasize institutionalization and sustainability of innovations into a health system, as opposed to just expansion of coverage (Zamboni et al., 2019). In contrast, sustainability refers to the extent to which an intervention can be continued beyond its initial implementation (Bonell, 2006). CE4AMR findings suggest that the relationships between acceptability, feasibility, scalability, and sustainability are not linear because both communities and AMR are dynamic (Mitchell et al., 2019). We propose that articulating approaches could offer a route to better understanding the potential for scalability and sustainability of interventions whilst also providing avenues to increase acceptability and feasibility in new contexts.
In this paper we use reflective discussions with team members on an active research project, to identify how and why articulating the specific approaches of PV and CDA could create a useful, and innovative methodology. We ask what happens when we bring these two approaches together, and we examine this articulation from the perspective of scale, sustainability, and longevity.
Hence, this paper aims to provide exploratory and methodological insights into the process of articulating PV and CDA, which is complex and challenging. We did not aim to provide a definition of articulation or a manual for its implementation. We acknowledge that our preliminary insights and reflections on the articulation process are not easy to pin down because of the intangible nature of this yet-to-be-fully implemented participatory approach. We also acknowledge that our reflections on the questions of scalability and sustainability are of an exploratory nature and face challenges related to language and interpretation of articulation. Our paper is about how participants in the reflective discussions have interpreted the articulation of the two participatory approaches from their own perspectives and the limitations of our paper show precisely the constraints related to a conversation between different disciplines and an effort to understand each other during the process. We relate this back to Hall’s understanding of the articulation process and the need for a situated/site specific/sociocultural approach to articulation.
This paper aims to demonstrate the need to reflect on the articulation of different participatory approaches across disciplines as an ongoing research question in itself that should be granted the space for exploration and not to be condensed into existing work that is finite and complete.
Research problem and rationale
This study aims to identify how articulating Participatory Video (PV) and the Community Dialogue Approach (CDA) adds values to individual approaches beyond the sum of their parts. These aims can be distilled into three discrete research questions.
-
How can articulating PV and CDA amplify the strengths and mitigate the limitations of each singular approach?
-
How can the two approaches (PV and CDA) complement and enhance each other in an interdisciplinary project?
-
How can the articulation of PV and CDA participatory approaches impact on the sustainability and scalability of an intervention?
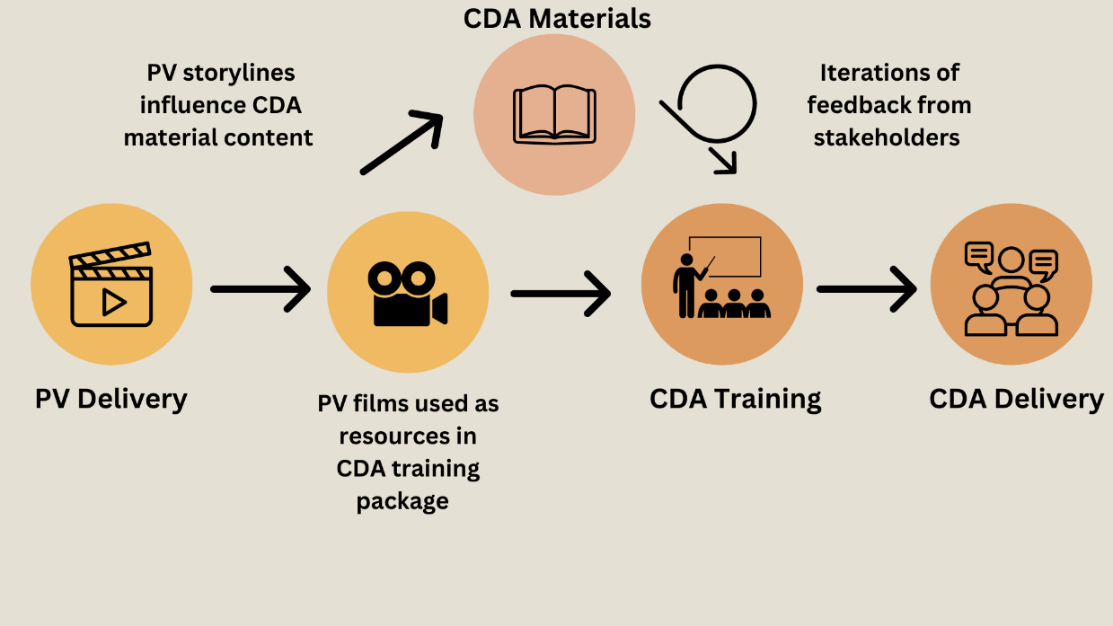
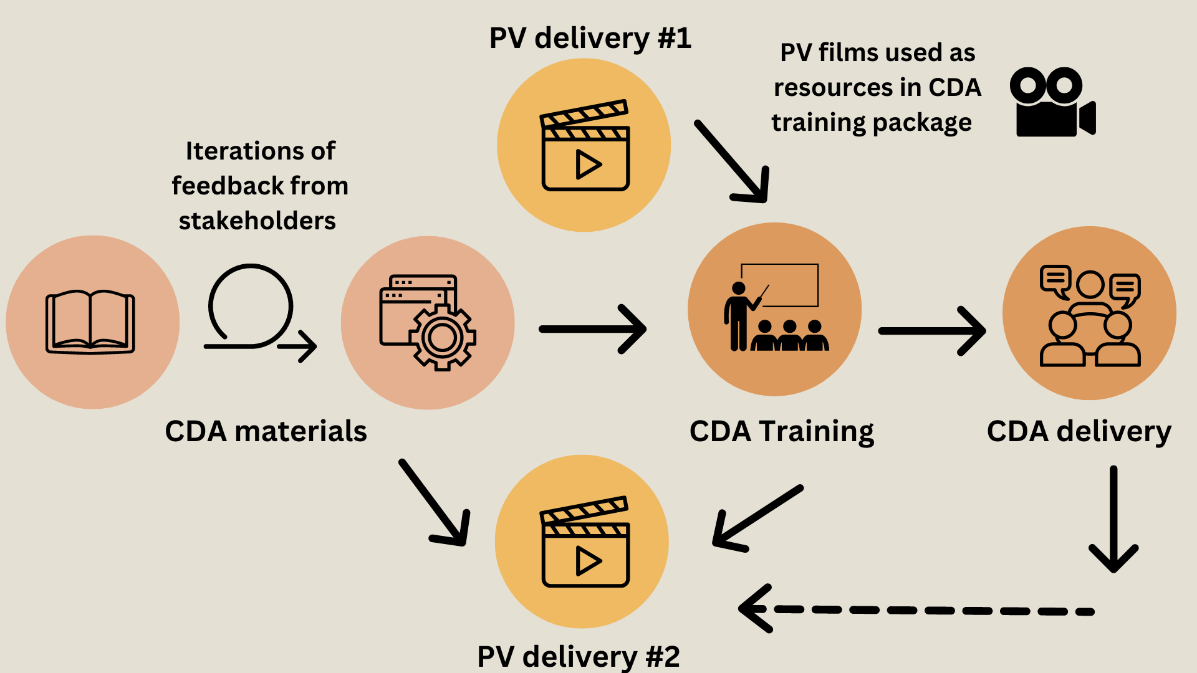
Within COSTAR, PV was planned to be the first intervention within each setting. Filmmaking was intended as a knowledge exchange opportunity to help research team members understand contextual details around One Health AMR challenges in each setting. Resulting films and storylines were anticipated to feed into the CDA materials thus making the overall COSTAR intervention co-produced and contextually informed. However, due to the COVID-19 pandemic and UK Official Development Assistant (ODA) funding cuts of 2021, (Richter et al., 2021) COSTAR suffered significant delays to field activities and this order of implementation was not quite possible. Figures 2 and 3 depict the delivery process of COSTAR within each setting. We focus on not just when each method of PV and CDA was delivered temporally but also where, why and how the two methods have intersected and informed each other within the wider COSTAR intervention. These could be depicted as cycle diagrams where both would have a gap or an incomplete segment, as presented in Figures 2 and 3.
In Nepal, the team was able to deliver two rounds of PV in 2022 prior to the development of CDA materials in 2022-23 (Figure 2). The film outputs thus directly informed the CDA materials, particularly by providing scenarios and character names for the stories used to exemplify AMR challenges. CDA material development stage began in January 2022 and ended in February 2023. This iteration of COSTAR will be evaluated in early 2025, the specific aims being to test the feasibility and acceptability of community engagement approaches in a rural, Tarai (plains) region of Nepal close to the open boarder with India.
_and_community_dialogue_approach_(cda).png)
In Bangladesh (Figure 3), however, there were significant changes to the delivery of the COSTAR intervention. Because Bangladesh’s CDA was evaluated via a cluster Randomised Control Trial (cRCT), the COSTAR team were constrained by strict timelines, meaning that post-COVID implementation had to focus on the CDA. The Bangladesh iteration of COSTAR was heavily informed by a 2018 pilot CDA study and household survey of AMR knowledge, attitudes, practices, and language. The COSTAR project conducted an additional baseline survey of community members’ One Health antimicrobial knowledge, attitudes, and practices in 2022 and an endline survey was planned to be conducted at the end of the CDA delivery phase (December 2023, while this paper was in the writing and review process). The CDA training began in Bangladesh in 2022 and was followed by an iteration of PV conducted in an area external but similar in context to the RCT delivery and control sites. The resulting films have deepened the teams’ contextual understanding of antimicrobial knowledge, attitudes, practices, and language within Bangladeshi communities and have been able to provide more contextually nuanced training materials but have not directly informed the CDA materials. In contrast the baseline survey and CDA training session were suggesting that AMR knowledge, attitudes and practices were highly likely to differ between urban and rural settings. As such the COSTAR team specifically conducted the second iteration of PV in June 2023 within a dense urban setting, to allow for comparison with the previous rural iteration.
_and_community_dialogue_approach_(cda).png)
It is useful to specify that PV did not start out as subordinate to CDA, but through the delivery of the project it has become clearer how PV best operates within the context of CDA. PV allows more in-depth investigation of a specific context in and of itself. This can then provide rich, contextually authentic stories for the CDA. The films can also provide useful trigger points for the development of CDA in different contexts precisely because they are permanent products that can be used in different contexts.
For example, the 2018-19 participatory video project (CARAN) which involved a number of the authors of this paper resulted in 6 short films considering local AMR challenges in two Nepali communities. These films were showcased to ward leaders and local government officials to demonstrate the AMR challenges faced by local people in an attempt to change policy. The films are available online, on the platform youtube, as part of the research project outputs. In the final film, Nisha’s Story, the HERD team (partners on both CARAN and Costar) return to one of these communities to catch-up with participants and consolidate their learnings around AMR. The film also won a diamond award (Short Doc) at the MindField film festival in November 2020. When engaging with these films the authors suggest the readers find out more about how to use the films as community co-produced resources in other contexts. These are direct community outputs, not health promotion tools and the content should be engaged with in the way the authors recommend.
Nepal was a pilot site selected for several reasons, one of them being in response to the funders call for research which looks at health and context – hence Nepal was brought in to see how context impacted on the CDA’s ability to diffuse AMR knowledge. There are also the specific challenges associated with the research team having the focal topic of AMR across One Health – there is very little knowledge about AMR at community level beyond drug misuse. PV offers an opportunity to explore this topic in much greater detail. This could have been a stand-alone project but because the information helped contextualise the materials needed for the CDA it seems logical to bring them together.
The co-authors of this paper agree that PV was not introduced as a means to support the development of CDA – rather that the outputs from PV seemed to provide rich and nuanced insights into the lived experiences of a community. In the case study of COSTAR, PV informed CDA – but it would be entirely possible for this to work in reverse in other settings or projects. As suggested elsewhere in the academic literature (Clarke, 2015), the act of articulation is always in flux, so the scenario presented in this paper represents one process only.
Reflective discussions
To answer the research questions, authors held reflective discussions with eleven researchers from across the COSTAR project’s partner organisations in the UK, Nepal, and Bangladesh. This team has mixed roles and different disciplinary backgrounds, as well as mixed genders and ages, allowing different perspectives on the process of articulation and its impacts which can broadly be defined as field/implementation insights, material development insights and academic or theoretical perspectives.
Reflective thinking and practice are often used by practitioners in various health and care related fields, professional services and those working in teaching and learning at different levels in the education system. In this paper we refer to reflective discussions as interdisciplinary and structured conversations where individuals reflect on their experience, skills and learning as part of the research projects where they used PV and CDA and their own understanding of these participatory approaches, both separately and when coming together.
The reflective discussions were conducted in-person between 6th and 10th March 2023 during an International Residential Writing Workshop in the UK. All discussions were filmed with recorded verbal consent given by the team member to the camera. The films were part of a larger visual communication project aimed at showcasing the work of the CE4AMR network in a Q and A format. The recorded consent is confidentially stored on a University of Leeds-owned server that is password-protected and only the research team members have access to it.
The reflective discussions lasted for 30-45 minutes, each participant taking part in one session at an agreed time and day that they had previous knowledge about and they could prepare for in advance, and explored three key questions: (1) ‘How are the PV and CDA elements coming together in COSTAR?’; (2) ‘Why is this important?’ and (3) ‘What is the goal of bringing these two methods together?’. Some of the participants also answered the question: ‘What are the relative strengths of CDA and PV?’. In their responses, participants added their own perspectives based on the role they had in the research project and their direct experience of working with PV or / and CDA in the field, or at the academic level.
Two researchers acted as interviewers (NJ and PC) with a project assistant, who provided support when they themselves were being interviewed. Interviews were then transcribed from video footage using the Microsoft Word dictate function. Two researchers (LG and JM) analysed transcripts using an inductive thematic analysis following Braun’s approach (Braun & Clarke, 2006). Researchers coded the interview transcripts manually to identify inductive codes, sub-themes and themes which were cross-checked between researchers and refined via extended discussions, meetings and whole-team reflections. Thematic analysis is a commonly used form of analysis in qualitative research that relies on structuring and organising the data, identifying reoccurring key words, terms and concepts, and categorising them into main topics, subjects or themes that are further refined and critically analysed in the light of the research context and relevant literature to help make sense of the information. Researchers are open and transparent about the analysis process and the challenges identified (Cai et al., 2022), which in this paper we refer to as constraints highlighted by the reflective discussions.
This article explores reflective discussions with existing research team members regarding their experiences of the COSTAR project so far. As such this work did not require a separate ethics application beyond the original approval granted by the University of Leeds Faculty of Medicine and Health Ethics Board (reference number: MREC 20-034). All participants to the reflective discussions provided free, informed, and verbal consent to be filmed, in the knowledge that their answers would be utilised to inform this article and several other research outputs.
Researchers’ positioning
The researchers who co-authored this paper were all part of the University of Leeds and the CE4AMR network and had different backgrounds and different roles in the research project at the time of writing this paper. [1] They have different levels of expertise across the fields of health, arts and natural and social sciences and have come to work together in this project as an interdisciplinary team.
Some of them are senior academics who designed the research, the COSTAR project and the PV and CDA approaches, while some were involved in the research process at different stages, including working directly with the CDA and PV material development and research participants in the local communities in the field, in both Nepal and Bangladesh. They have built a long-term relationship with the stakeholders in the countries where the research was conducted and have met directly with the participants in the PV and CDA sessions in-person during several field trips. One of the co-authors joined the team later and was specifically involved in the co-production of academic outputs from the COSTAR project and has met all the participants to the reflective discussions in-person as well as during regular online meetings, getting to know the background of the research and leading the writing process.
Key themes
Three key themes emerged from the data in relation to articulating the approaches of CDA and PV. Themes emphasize that their articulation (1) amplifies co-learning beyond the individual benefits of knowledge exchange associated with each approach individually, (2) adds value that complement the potentials of each of the two participatory approaches separately and helps to overcome their individual shortcomings and (3) magnifies ownership as a key tool for the community to have control over what and how to narrate their views on AMR and how to represent the narratives that emerge as ‘their own story’. The constraints identified in connection with articulating PV and CDA were mainly focused on the provision of resources in the field, such as time and logistics. We will return to reflect further on this point in the Discussion section.
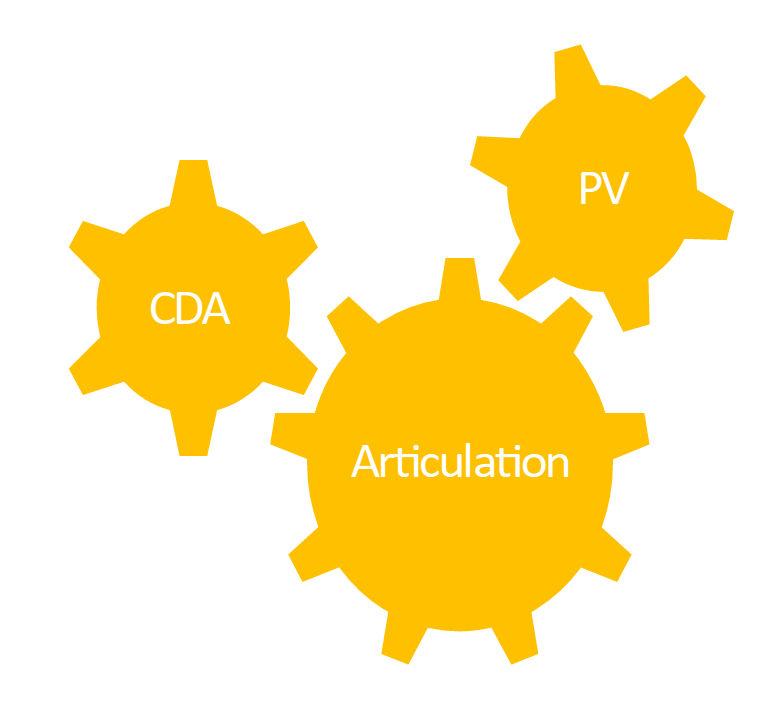
A visual representation of articulating PV and CDA is available in Figure 4 below, as an imaginary circle with three gears, suggesting a way of working together that involves ongoing dialogue and interaction between the three parts involved, as well as the idea of incompleteness and potential limitations or constraints that define such interactions. This illustrates that each is an intervention in its own right and not inherently connected, but that by incorporating the idea of ‘articulation’ we can make the two move harmoniously – creating a larger impact than if each were to ‘move’ alone.

Theme 1: Articulation amplifies Co-learning
It is important to mention at the start that articulating CDA and PV constitutes an integrative part of the broader Community Engagement (CE) approach used in COSTAR in which communities identify local issues and co-develop local solutions (King et al., 2020). In this respect, co-learning involves adopting a dual route of knowledge sharing which includes exploring together and learning together.
PV and CDA are taken as an approach of community engagement and both are supposed to help in some way understand the issues of AMR and try and identify some solutions…, and addressing the local issues and developing a local solution to the issues. (P6)
At the level of the health intervention in Nepal and Bangladesh, participants in the reflective discussions felt that articulating PV and CDA amplifies co-learning in training and dialogue triggering, for instance by using the outputs from PV in the process of training the trainers who deliver the CDA to ‘prompt dialogue and discussion around issues connected to AMR at community level, and that has been a really useful aspect of articulation.’ (P1)
Articulating PV and CDA has been an approach in the making for the past four years, and the CE4AMR network has developed an open perspective towards it, maintaining an open mind about the utility of this new approach and allowing for questions about the possibility and acceptability of articulating the two approaches to emerge organically:
We weren’t really sure exactly how they (PV and CDA) would fit together and I almost think that was the goal, to question quite openly can we articulate these methods? Is it possible? Is it reasonable? Is it accepted? (P4)
Upon further reflection, the participants added that the authorship team wanted to be open about the possibility of articulation of the two approaches, but not be driven by finding a way to ‘make it work’. Through COSTAR we are genuinely asking ‘can these methods work together’ and what really happens when we articulate them. The use of PV outputs to inform CDA materials in Nepal was the most direct example of articulation where the researchers felt they could clearly say ‘yes, these approaches directly fit together’. Asking a wider group of participants-researchers to share their reflections on the articulation of the PV and CDA was meant to produce more balanced feedback, and to be open to other interpretations. Hearing from multiple people working on the project allowed the experience of planning and delivery to be captured and reflected upon.
Moreover, joining the two methodologies with the aim of amplifying co-learning also means that adaptation is a key tool that enables the narration of local stories and local meanings, since both PV and CDA are participatory methods which involve co-creation by the community:
*CDA also includes participatory activities so we have a story; that is the story based on the discussion we had when we do the CDA dialogue approach. So the story has been adapted from the PV work that has been done (P6).
These interlinkages then amplify the aims of each approach, for instance by using PV to learn about the issues in the community and ‘using those findings to develop the content of CDA’ (P1). But the articulation of PV and CDA goes beyond this by providing space for innovation and creativity: ‘as the project has progressed, I have come to understand that we can link these two approaches in much more creative ways’ (P1). This will be exemplified in theme 2.
Theme 2. Articulation can add significant value to each method and mitigate shortcomings
By articulating these two approaches, we aim to understand their benefits but also ‘the mechanisms of change in each of these different approaches’ (P2). As a result, articulation adds value in the following ways:
Complementarity: ‘the use of PV has been enormously helpful to inform the CDA itself.’ (P6).
Effectiveness and Innovation:’ we are looking at how to take the best of different approaches to community engagement in order to try to do something that is really effective and innovative. (P2)
Sustainability: ‘by bringing them together it allows us to do something that is both sustainable and scalable in a way that neither of the approaches are on their own’ (P2).
Scalability: ‘So those videos themselves do not necessarily have this kind of educational output on their own, but that they can be used to show the participants from different areas to ask what they see in those films in a way that is very practical, that can be replicated and shared.’ (P5)
PV is a mobile resource that can be transported into other settings, so it does not only allow people ‘to articulate the problem for themselves but also to take that problem into another context where they might find it useful.’ (P2). However, this point requires further reflections on the possible constraints involved in the mobility of PV. To share videos requires a set of resources that are not always available. PV has the potential to be shared widely but only where resources allow this to happen, whereas CDA requires much less technical resource to be delivered.
PV is also a form of participatory learning, where making the film is just the starting point, and this needs to be followed by an impactful outcome: ‘It is about making films and making sure that those films are played to the people that can support the community to affect change or to affect the changes that they want’ (P2). This value speaks about the potential for change and impact at different levels, including political and policymaking, locally and nationally, as one of the participants mentioned when reflecting on the use of PV: ‘[You can] use your videos to talk to policy makers and local authorities’ (P3). Or, as explained from an example about a PV film made by a community in Nepal and shown to policy makers at a policy-oriented event, the films are considered to have power to engage policy makers in considering the potential of the community as agents of change that it is worthwhile engaging with:
And again it was the fact that basically, policy makers have really low expectations of their voters, so the fact that people got together to make these films, basically saying ‘this is what the problem is, from our point of view’, is really powerful because it is saying ‘‘Oh, we need to really listen to it, if they can get their act together to do that, maybe they can vote us out of power’’'. (P2)
On the other hand, PV has shortcomings in terms of being resource-intensive, ‘labour intensive and expensive getting cameras together, doing the training.’ (P2)
*It is not a project that you could replicate over and over and over again. It’s quite resource intensive. It’s also not necessarily very helpful to just constantly be making different videos of similar sort of things (P5).
CDA as a stand-alone approach has its own strengths which include being less resource intensive, and not requiring the kind of logistics and equipment such (cameras, microphones, sound recorders and so on) that PV does. However, some of the participants reflected on the fact that the CDA has its own weaknesses, especially its temporariness as an intervention: ‘you have to reinvent it every time you do it so there is less permanency’ (P2). However, on further reflection, other participants (P1) disagreed with this point, asking in what way CDA is temporary and being reinvented every time. P1 reflected on how each CDA is distinctive in its delivery. However, they highlighted how the purpose of COSTAR project was to create the CDA as a permanent structure within the health system. Hence they did not perceive this as a weakness. Other participant (P5) highlighted the distinction between the CDA more widely, a hopefully permanent part of the health system, and the actual CD sessions which are temporary, live and finite each time. The debates surrounding what is considered a strength and what is seen as a weakness and by whom will be further explored in the Discussion section.
Theme 3. Articulation magnifies ownership
Participants emphasised that they saw the articulation of PV and CDA as a potentially useful way to increase their understanding of AMR and their sense of ownership over the proposed solutions to this issue.
The community could feel the ownership of that complex health issue, they could see that ‘yes, this is us, this is our story, we should be more aware about this, we should be more focused on it’. That’s why I think these two (PV and CDA) should be joined together (P6).
Hence, articulating PV and CDA means asking how these two participatory approaches can be used together and for what kind of outcomes. Articulation is then a process with the key aim ‘to explore genuine community perspectives’ (P5).
Using those tools and outputs that participants have had a real say in making, so participants get to review the footage that they have made, they get to edit parts of it, and then they get to control every narrative that they put out, and to reflect on their own practices so they can share stories that mean a lot to them. (P5)
The idea of community ownership is part of the PV making process, frequently described as a process of ‘co-production’ and co-decision making: ‘a kind of collaborative experience where participants and film makers get to co-produce content in films and then decide how those films are shared afterwards.’ (P5)
CDA includes the concept of ownership in the sense of participants and facilitators engaging in a discussion about the issues identified by the community and ‘building together a solution that works for them, that is contextually and locally appropriate for that community’ (P9).
Constraints of Articulating PV and CDA
Several constraints were identified during the reflective discussions regarding implementing the articulation of PV and the CDA in both Bangladesh and Nepal. These were related to resources, time and logistics. Participants highlighted: ‘We do the best for us to show the PV videos to the community during the CD, we plan that initiative, you know, but given the resource constraint we could not do that’ (P9).
We have got lots of suggestions, like how it (PV) can be articulated with the CDA at the field level. But for the logistical support I think it requires huge logistical support to show the PV output in the field so that people can understand how they can identify the solutions along with the CDA. (P8)
Further exploration of the constraints will be explored in the Discussion section of the paper.
It is important to note that the reflective discussions were designed to capture the co-authors personal experiences and interpretations, rather than act as a means to reflect on the wider literature.
Discussion
This paper aimed to explore: 1: How can articulation of PV and the CDA amplify the strengths of each approach? And 2: How can articulation of PV and CDA mitigate the limitations of each approach?
It used reflective discussions with members of an active Community Engagement project to identify the merits and challenges of articulating PV and CDA approaches. Findings reveal that articulating PV and CDA can add value to each approach, beyond the sum of their parts, by amplifying co-learning opportunities, mitigating the shortcomings of each individual method and magnifying community ownership. However, each approach individually, as well as the process of articulation itself, demand specific resources which could be considered constraints to the process of articulation.
The aim of this paper is to consider the methodological potential of how articulation can amplify and mitigate methodological strengths and weaknesses. In the absence of a specific framework we decided to use the common values and principles that underpin the community engagement (CE) approaches to tackling AMR identified by the CE4AMR projects from a previous piece of work (Mitchell et al., 2019) to guide the discussion.
This specific piece of work is relevant here for two reasons: first, because it presents seven values underpinning the application of Community Engagement (CE) approaches to the One Health challenge of antimicrobial resistance (AMR). These values helped to frame the theoretical direction of COSTAR. And secondly, it was developed using a similar methodological framework to the current paper: based on reflective discussions with 40 interdisciplinary researchers during an international workshop in June 2019, at the beginning of the CE4AMR network from which the COSTAR project evolved. In the 2019 workshop and the resulting publication the researchers defined a value as a quality or standard which a CE project is aiming for, whilst a principle was an objective which underpins the value and facilitates its achievement. The values of Clarity, Creativity, Evidence-led, Equity, Interdisciplinarity, Sustainability and Flexibility were identified by a network of 40 researchers and practitioners who utilise CE approaches to tackle complex One Health challenges.
The three themes identified in this paper (amplified co-learning, adding new values, and mitigating shortcomings and magnified ownership) relate well to the common values and principles of CE approaches and the strengths and limitations of each individual method discussed in this paper often link back to our defined values and principles for Community Engagement approaches more generally. This shows an interesting connection between the work we carried out at the start of the COSTAR project and our thinking as we near its end. Thus, the project has come full circle in the sense of linking its values and principles in a creative and innovative way and exemplified here in the articulation of the PV and CDA approaches.
For instance, the value of creativity is about including artistic practitioners in the co-production team and in this paper we evidence that articulating PV and CDA amplifies the creativity of the approaches as both are participatory methods which involve co-creation by the community.
The value of an evidence-led approach to CE methods refers to valuing the expertise and lived experience of the community, and how the evidence can best be shared and made accessible after the project is completed (Mitchell et al., 2019). This is connected to the values of sustainability and ownership, which are about the ethics around what happens to a project when the funding ends, ensuring communities have strong ownership of a project, allowing them to visualise how resources and skills could be used beyond the funding lifespan (Mitchell et al., 2019).
This also means that the key to achieving impact are the concepts of feasibility, appropriateness for context, scalability and sustainability. For instance, to ensure that the intervention a project such as COSTAR develops is feasible, appropriate to the context, scalable and sustainable, and hence more likely to be adopted nationally, the research team worked closely with local stakeholders and research organisations to involve Ministry of Health and District Authority officials and their development partners in the project in Nepal, since they play a vital role in shaping policies and resource distribution. They are best placed to know the realities and constraints of the health system within which the intervention must be integrated and their views have been captured in the co-development of the PV and CDA materials, as explained in the earlier sections of this paper.
Furthermore, in our paper we emphasize the importance of articulating the PV and CDA to amplify the value of the individual strengths of each participatory approach that include narrating local stories in a contextualised manner. This then complements the strengths of both approaches and mitigates the issues around scalability and sustainability frequently discussed in the literature around such approaches by magnifying the sense of ownership that the community has over the stories they co-create, produce, script and represent. And this point is also related to the concept of co-learning, evidenced in the first theme in the findings. We used this concept to help us reflect on the idea of knowledge exchange that was reoccurring in the reflective discussions. The researchers from the CE4AMR network have been using the concept of knowledge exchange for years in relation to specific methodologies used for Community Engagement. However, when discussing the articulation of the PV and CDA in this paper, the participants referred back to terms such as co-learning, co-development, mutual learning. Hence this has led us to reflect on how articulating two participatory approaches can soften the transactional nature of knowledge exchange by allowing different communities and stakeholders to use different routes to share and develop different kind of knowledge(s) and to co-develop new knowledges. Or, in the words of one of the participants:
We first go into the community and understand what their practices are around the topic. And then gradually sort of learn from them and you know, engage in an approach where they understand what we are trying to deliver in our messages through various sessions… So that is how there is this mutual learning [in the articulation of PV and CDA] (P.11).
We also acknowledge the value that interdisciplinarity has across the CE methods and in understanding the experience of different team members from across multiple disciplines so that learnings are shared more widely (Mitchell et al., 2019). In the spirit of the same key value, in this paper we use the reflective discussions with ten team members from across disciplines and international teams to highlight the potential and values of articulating CDA and PV in health interventions in Nepal and Bangladesh.
Finally, the value of flexibility is key to the CE method, which is an iterative approach in nature, allowing stakeholders to modify methods and outputs as they learn throughout the project (Mitchell et al., 2019). Flexibility is also a key component of the PV process and the CDA: both methodologies take an active/reactive approach to the needs and priorities of the community they are based in, and both can adapt according to learning in real time. For example, the workshop phase of PV is led by the participants, as are the outputs and settings for showcasing the films. In a nutshell, the core components of each method remain the same in each project, but each looks differently in practice, depending on the ways the community shapes them. Likewise, we reflect in this paper on the importance of iteration and flexibility in articulating the CDA and PV across disciplines, while having its own constraints, and acknowledging the ‘not yet finished’ nature of such participatory approaches, which can be thought about as a ‘carousel of moving methods’ (Duggan, 2021).
In terms of the constraints of articulating PV and CDA, such as resources, logistical support and time, that participants mentioned in the reflective discussions, we acknowledge that these need to be considered in the wider theoretical framework and at the implementation stage of each project. For instance, it is very important to try to understand the needs and priorities of the setting in which the project is to be implemented, before the implementation stages. There are likely to be complex constraints to implementation that must be mitigated in contextually appropriate ways. In such cases, the planning and sensitization stages might need to take longer than one might need when employing a single form of CE approach if one is to engage meaningfully with the communities and the stakeholders that can help to mitigate any challenges during the implementation stage. Our paper acknowledges that CE interventions are resource heavy in terms of time, personnel, financial requirements and other resources, which is at the same time an inherent part of a research process and acknowledged when using other approaches, too, such as trials.
We have come to understand that CE methods on their own are resource-intensive and by default articulating participatory approaches is going to increase the resources required, particularly in terms of time and interdisciplinary skillsets required within the team. However, the benefits of articulating participatory approaches appear to provide more value and create more agency for the participants as evidenced by the three key themes that we presented and discussed in this paper. Evaluation data will be able to shed more light on this aspect from the participants’ perspective which might, in turn, offer possible new directions for future research.
The research team has also come to understand that ideas around the articulation of PV and CDA are constantly in flux, and they depend on context, language and interpretation. These ideas face challenges in terms of different uses of language by different participants situated in various disciplines and having different backgrounds, as explained in the earlier sections of this paper. For instance, some of the participants have a different perception of the temporal nature of an approach and perceive some other approaches to have more longevity. While other participants have been academically trained to think about methods in the sense of processes and systems. For instance, if we think of the CDA primarily in terms of the actual CDs themselves, then the outputs are quite temporary (live) sessions that need to be repeated live each time, but if we think of the CDA primarily as a process with live elements then it might be easier to see it as a permanent approach to be embedded into larger systems. Hence, what some participants consider a limitation from the perspective of their discipline is seen as a strength by another participant coming from a different background. Moreover, some participants perceive constraints such as time and resources as limitations in implementing the articulation of PV and CDA, while for others these represent more of a logistical reality that needs to be acknowledged and it can always be present in a research setting.
In their paper about the challenges of interdisciplinary research, Daniel et al. identified some of the key mechanisms that enable researchers across disciplines to work together and to learn from each other, as well as to acknowledge the challenges they face (Daniel et al., 2022). Some of the mechanisms for collaboration include reflection and transformation, where reflection is the process of identifying how and why practices are different. Transformation is a concept that captures changes in practices, and potentially leads to the creation of a new interdisciplinary collaborative practice. Some of the challenges mentioned are related to language inconsistencies across researchers from varying disciplines that impact communication, such as jargon and the lack of understanding of some terms by collaborators, which then create the need to provide definitions. This has been acknowledged elsewhere, too: ‘scientists trained in a discipline learn to speak a specific language and adopt the analytical and methodological constructs that have accumulated in that discipline’, which can be an obstacle to interdisciplinary research (Pellmar & Eisenberg, 2000).
Different disciplines also have differing methodological/theoretical approaches and standards due to conflicting disciplinary paradigms. In this case a valuable starting point to overcoming conflicting paradigms can be to first clarify backgrounds for bridging differences by sharing different perspectives and being more explicit about the assumptions that everyone holds (Daniel et al., 2022). Communicating with another discipline requires time and work. An extensive effort must be made to learn the language of another field and to teach others the language of one’s own (Pellmar & Eisenberg, 2000).
We feel that the methodological reflections in this paper make a valuable contribution to the efforts that researchers across disciplines make to enable learning from each other and working across cultures, disciplines and paradigms to co-produce innovation and transformation in the field of participatory research methods.
Outlook
This paper provides preliminary and exploratory methodological reflections into the articulation of two different participatory approaches of Community Engagement across disciplines: Participatory Video (PV) and Community Dialogue Approach (CDA). Our findings that emerged from conducting reflective discussions with researchers-participants show first, that articulating these two participatory approaches can offer rich potential for amplifying co-learning between community, stakeholders and researchers. Secondly, articulation adds value by complementing the strengths of each approach and mitigates their shortcomings. Thirdly, articulation magnifies the sense of ownership for communities to co-create, produce and represent their stories via the articulation of PV and CDA. The articulation is a complex and not yet finished process which brings its own challenges and constraints for an interdisciplinary project, and we suggest the need for further exploration, critique and reflection.
Authors’ contributions
JM, NJ, PC and RK designed the study. LG led the paper writing process. PC and NJ conducted the reflective discussions. JM and LG conducted the data analysis and wrote the findings. PC, RK, JM, NJ contributed to reviewing the paper. All authors agree with the final version of this manuscript.
Funding details
This work was supported by the UKRI’s Medical Research Council Grant number MR/T029676/1.
Disclosure statement
The authors have no known conflict of interest to report.
Acknowledgments
The authors are thankful to our team member, GP, for her valuable contribution in conducting and recording the reflective discussions for this paper. The authorship team would also like to thank The Medical Research Council who funded the COSTAR project.
In early 2024, after this paper was accepted for submission but before its publication, two of the co-authors have taken a new research position and moved from the University of Leeds to another academic institution in the UK.