Introduction
Health inequities can be amplified when members of the community are not directly involved in research (Brush et al., 2020; Cacari-Stone et al., 2014; Ward et al., 2018). Community-based or engaged research involves a set of approaches and methodologies to more effectively engage lay community members in research regarding their own experiences, health, and well-being. To start, clarifying what “community” means is essential at the outset of any community-engaged research project initiative. The idea of community and ways it is operationalized tends to focus largely on the participation of community-based organizations that serve the populations of individuals that researchers are most interested in engaging. In health equity research, this often takes the shape of academic-provider, academic-community based organization, and academic-municipal partnerships (Bowen et al., 2017; Brush et al., 2020; Caron et al., 2015; Coombe et al., 2018).
In academic-provider engaged research, hospitals, clinics, and federally qualified health centers work in partnership with large research institutions to answer a research question through traditional studies, or set out to establish community advisory boards or commissions to inform decisions made by the healthcare institution (Duran et al., 2019; Kegler et al., 2016). This is also true for academic-municipal partnerships, in which a state or local department of health or school system typically partner with an academic research center (Kegler et al., 2016; Ortiz et al., 2020). This is distinct from most academic-community based organization (CBO) research projects, where the academic partner tends to be the entity that reaches out to the CBO for assistance or to gain input and advice from staff (Duran et al., 2019; Kegler et al., 2016; Ortiz et al., 2020). The community-engaged research project is, therefore, impacted by the entity conducting the initial outreach for partnership as the partners they engage with will align with their own understanding of community. A 2001 study aimed to survey several health equity researchers and concluded that due to the wide range of methods that might be used in community-based or partnered research, the definition of community should ideally be decided upon for each individual study (MacQueen et al., 2001) (emphasis added).
In our experience with community-engaged research, we have found that the relevant communities to engage will vary both based on the research objectives as well as the respective partners’ interest, primary missions, resources and skill-set (Romero, 2020). Ideally, the communities, or stakeholders, engaged and the nature of their engagement will be negotiated to reflect their respective priorities and contributions to the project. When developing the study design and recruitment plan for this research project, we defined community broadly to enable engagement of the diverse stakeholders impacted by healthcare segregation in New York City (NYC) through a variety of recruitment modalities. To address research questions regarding New Yorkers’ experiences with healthcare segregation, we iteratively engaged with community members, or stakeholders, from municipal, academic research, civil society, and corporate sectors, in keeping with qualitative inductive approaches to study implementation and data collection (Corbin & Strauss, 2015; Glaser & Strauss, 1999).
The project’s focus on healthcare segregation and health inequities made it an ideal topic for community engagement given the history of segregated access to healthcare and discriminatory experiences in New York (Calman et al., 2006; Dunker & Benjamin, 2020; Tikkanen et al., 2017) and associations with health disparities (Attanasio & Kozhimannil, 2017; Call et al., 2023; Grady & Ramírez, 2008; Han et al., 2015; Kaiser Family Foundation, 2022). Several policy decisions over more than 30 years have contributed to hospital segregation, such as deregulation of payer rates to hospitals resulting in higher reimbursement rates to private hospitals, and inadequate allocation of the state Indigent Care Pool to safety-net hospitals despite their serving more Medicaid and uninsured patients than private hospitals (Calman et al., 2006; Dunker & Benjamin, 2020). While there is clear evidence of current healthcare segregation by race/ethnicity and insurance status in NYC (Tikkanen et al., 2017; Zhilkova et al., 2023), a coalition of researchers, community partners, and healthcare providers in the Bronx documented a system of medical apartheid associated with healthcare and health outcomes disparities almost 20 years ago (Calman et al., 2006). Individuals who report negative experiences accessing care or treatment are less likely to return for follow-up care and are more likely to experience negative health outcomes than individuals who had neutral or positive experiences seeking care (Attanasio & Hardeman, 2019; Attanasio & Kozhimannil, 2017; Hsia & Zagorov, 2022). In addition to these experiences being associated with worse outcomes related to a prior hospital visit, it can impact an individual’s future health by making them more likely to delay, stop, or disengage with healthcare altogether (Attanasio & Kozhimannil, 2017; Nong et al., 2020; Selvarajah et al., 2022).
To gain a better understanding of care segregation and how it impacts New Yorkers, we set out to recruit New Yorkers from across the five boroughs to participate in focus group discussions regarding factors associated with hospital choices and healthcare experiences among people of different racial/ethnic identities and health insurance statuses. The goal of this methods-focused paper is to present our broad definition of community and how we employed an iterative and expansive approach to community-engaged recruitment with stakeholders from four different sectors within a large qualitative research project.
Methods
Community-engaged Approach
The Health Equity and Access to Care (HEAC) Project used a multi-faceted community-engaged approach to learn about New Yorkers’ healthcare experiences and the extent to which this might vary across individuals with different racial/ethnic identities and health insurance statuses. The project ultimately aims to articulate a set of programmatic and policy recommendations for reducing inequitable and segregated healthcare in NYC. The project methodology employed engaging with an interdisciplinary set of communities across the city in order to collect data directly from a diverse sample of New Yorkers (via focus groups) about their experiences obtaining healthcare in hospitals across NYC, as well as insights from organizational stakeholders (key informants) who engage with New Yorkers around healthcare. This involved a strategy that utilized a variety of outreach and data collection methods with a wide range of stakeholders from different sectors, or communities, across New York City. We intentionally employed an integrated community engagement strategy that allowed for the myriad ways in which different communities could both contribute to project recruitment efforts as well as participate in the project. This fostered ongoing and bidirectional communication between the community-based entities and research project staff, such that recommendations from the specific data collected were integrated throughout the project and led to additional communities being included, among other things. This community-engaged recruitment approach was balanced against the methodologic goal to recruit New Yorkers from all over the city, irrespective of their connection (or lack thereof) to specific providers or other community stakeholders. In other words, we engaged with a wide array of stakeholders interested in assisting with recruitment, while ensuring that it was not limited to the New Yorkers they served so that we could capture the broadest range of healthcare experiences.
Participant Eligibility and Informed Consent
To participate in a focus group, respondents had to be 18 years of age or older; reside in one of the five NYC boroughs; have obtained or tried to access either outpatient or inpatient care at a hospital in NYC in the past 12 months; primarily identify within one of four broad racial/ethnic categories (Black/African American [B/AA], Hispanic/Latinx [H/L], White/Caucasian [W], Asia/Pacific Islander [A/PI]); and have health insurance to compare participants with private/commercial and public/Medicaid health insurance. Key-informant interviewees were relevant stakeholders such as hospital administrators, health advocates, community-based service providers, and health program staff who could speak to issues regarding healthcare access in NYC from professional experience. Informed consent forms were signed and submitted digitally or in person by focus group participants and key informants, and all were given $50 for their participation. This project was approved by the City University of New York (CUNY) Institutional Review Board (IRB) on June 15, 2022 (#2022-0401-PHHP). All research project staff had current CITI certification in two or more of the modules on ethical and responsible conduct of research.
Data Collection
Screener and post-focus group survey
Individuals interested in participating completed a brief screener administered via Qualtrics or in person (with a CAPTCHA element to reduce the likelihood of non-human completion), which allowed us to determine eligibility for focus group participation, collect demographic information to describe the participant sample, and track ongoing outreach and recruitment efforts. We developed a post-focus group survey to augment the qualitative data with information regarding participants’ experiences with health-seeking behaviors; healthcare/hospital experiences; and healthcare/hospital preferences. Both the screener and post-focus group survey were administered through the Qualtrics platform.
Focus Groups
Focus groups allowed individuals to describe their experiences accessing healthcare in detail. Moreover, the interactive nature of focus group discussions often generates additional information that individual interviews alone generally would not yield (Morgan, 2019). We collaboratively developed the focus group topic guide with our health department colleagues, informed in part by their analysis of NYS SPARCS hospital data (identified significant differences in discharge from private vs. public/safety-net hospitals by patients’ race/ethnicity and health insurance status) as well as by our literature review of salient issues related to accessing healthcare. We subsequently shared it with all other collaborators (described below) throughout the project to allow for further input and revision. The topic guide contained 11 open-ended questions pertaining to participants’ experiences accessing and/or attempting to access care categorized into five domains: 1) choice of facility/finding care; 2) factors affecting healthcare experience; 3) specific healthcare experiences; 4) healthcare in NYC; and 5) experience with specific scenarios. As is typical of qualitative data collection, the topic guide was revised as focus groups were conducted and the wording and order of questions were refined, keeping with inductive grounded theory methodology (Corbin & Strauss, 2015; Glaser & Strauss, 1999). Once eligible participants were identified through the screening process, we coordinated real-time virtual focus groups with participants (approx. 4-6) stratified by race/ethnicity and insurance, for a day and time that worked within their collective availability (morning, afternoon, and evening time slots, Monday to Sunday). The two-hour focus groups were initially conducted online via Zoom (in light of the COVID-19 pandemic) but later focus groups (when there was a lower risk of infection) were also conducted in person at partner CBO sites. All focus groups were digitally recorded, transcribed and uploaded to Dedoose.com for analysis.
Key Informant Interviews
To explore issues raised by focus group participants and emergent themes, we conducted key informant interviews (KIIs) with relevant stakeholders in their professional capacity (described above). The semi-structured interview guide contained 12 open-ended questions that addressed their clients’ experiences with choosing healthcare facilities/finding care, factors affecting specific healthcare experiences, and their professional insights on the most important issues to consider and how healthcare can be improved. The one-hour interviews were conducted via Zoom video conference, digitally recorded, transcribed, and analyzed in Word.
Defining “Community” for Collaboration and Project Recruitment
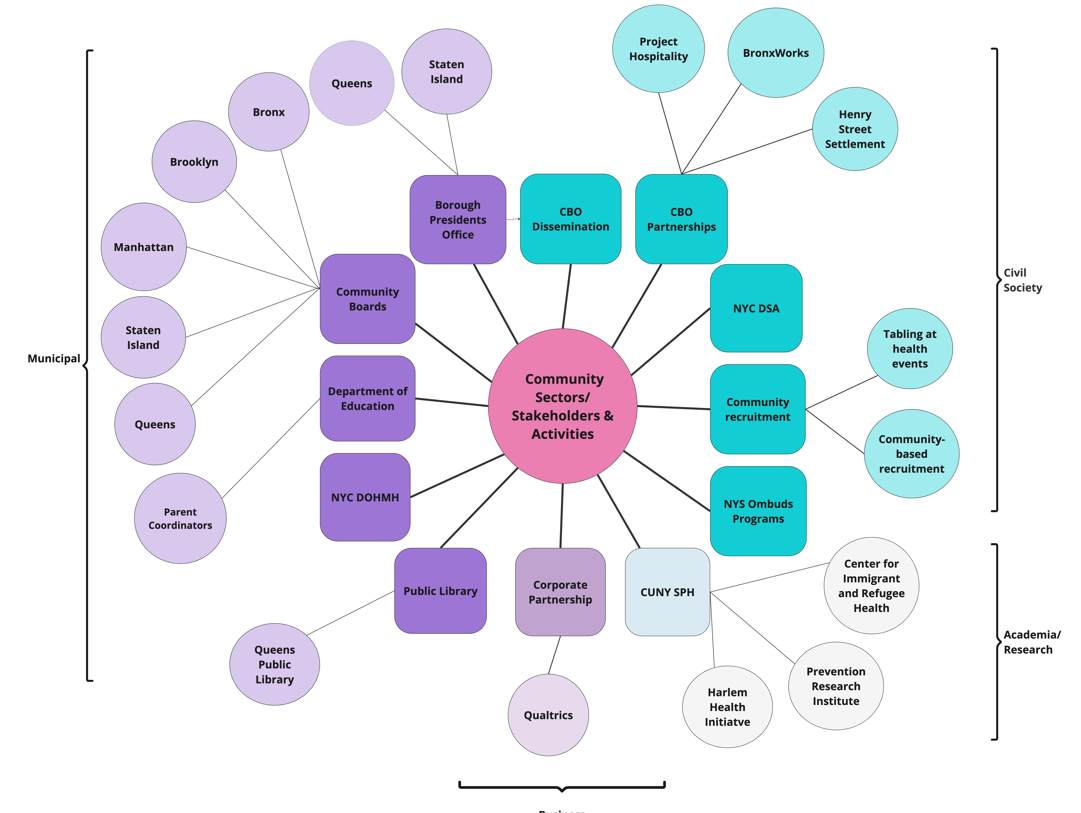
In order to reach and include diverse New York communities in this project, it was essential to work with four key sectors, including civil society, academic research, business, and municipal institutions. From the outset, the HEAC focus group study goal was to engage a diverse set of New Yorkers from the five boroughs, with different racial/ethnic identities, Medicaid or private insurance, who had tried to access care at a hospital in the past year — an ambitious undertaking. While it would have been much easier and required fewer resources to solely partner with a limited group of organizations and conduct focus groups with the individuals they serve, this would have substantially limited the range of New Yorkers participating and the data collected regarding their healthcare experiences. For example, collaborating solely with service-oriented CBOs would have limited recruitment to those already engaging with these entities and not provide a complete picture of New Yorkers’ experiences with healthcare. As such, the inclusion of other key stakeholders was critical from both methodological and substantive perspectives. That said, the healthcare sector was not included as we sought to avoid bias from recruiting those specifically in contact with healthcare facilities.
We employed a phased recruitment strategy starting with broad-based outreach through various stakeholders within three of the four main sectors (i.e., municipal, civil society, academia) (Figure 1). This allowed New Yorkers to learn about the project through countless means given the vast potential for information dissemination through different organizational communications modalities, including social media. Within these sectoral categories, we further engaged with numerous stakeholders interested in the health of New Yorkers. As such, we employed an inclusive multi-sectoral community-engagement approach that allowed for a broad definition of community (Figure 1). Below we describe the network of diverse stakeholders we engaged with for project recruitment and participation within their respective sectoral categories.

Municipal Institutions
Department of Health and Mental Hygiene (DOHMH): The NYC health department provided funding for the project and served in a valuable collaborative role assisting with study design development, review and input on the data collection instruments, and contributing insights on the ongoing data analysis process. They assisted with recruitment by sharing project materials with their community-based grantees, city vaccine and COVID testing sites, and green market programs.
Community Boards (CB[1]): We reached out to all 59 NYC community board presidents and district managers via email about the project and followed up via telephone. In addition to sharing project materials to be distributed to all New Yorkers in their respective districts, we asked to make presentations about the project at relevant health-related committees (e.g., Health and Human Services sub-committee) and general board meetings with the public. We were able to do so with approximately half of these stakeholders (n=26) over a six-month period. In these meetings, community board members encouraged participation in the focus groups and the district managers distributed recruitment materials through the CB websites and email lists.
Borough Presidents (BPs): We contacted the five NYC borough presidents via emails and direct phone calls to disseminate the recruitment materials to their constituents and request meetings with relevant staff to introduce the project and elicit feedback. This led to meetings with staff from two of the BP offices and resulted in their disseminating recruitment materials through their borough-wide channels as well as suggesting potential community-based partners who could further assist with recruitment.
Department of Education (DOE): One of the many recommendations resulting from engagement with the community boards was that we reach out to School Parent Coordinators and Wellness Coordinators at the NYC DOE. Despite the lack of a centralized directory for individuals in these positions, we emailed recruitment materials to coordinators at 75 schools based on exhaustive research for their contact information across the 32 NYC school districts.
Public Library Systems: Given the community-based nature of libraries (Klinenberg, 2018), we explored the possibility of community engagement with the three public library systems in NYC (New York Public Library [NYPL] serving Manhattan, the Bronx, Staten Island; Queens Public Library [QPL]; Brooklyn Public Library [BPL]). We succeeded in sharing recruitment materials with the QPL via their Community Health Coordinator for consideration by their legal department but were informed of a policy that prohibits the library from sharing information with the community that involves compensation (i.e., the study incentive) irrespective of the source (academic; non-profit) and nature (healthcare equity; public health) of the activity. As such, despite their interest in health equity, they could not assist in disseminating materials to the communities they serve.
Civil Society Groups
Community-based Organizations (CBOs) and Partnerships: We conducted multiple rounds of broad-based outreach sharing informational materials with upwards of a hundred CBOs that engage with communities and provide social and health-related services. We and/or collaborating organizations had pre-existing relationships with many of these CBOs. A separate CBO-focused effort involved identifying approximately four organizations in each of the five boroughs concerned with health equity in their communities that had the interest and ability to partner in focus groups involving their community members. Several CBOs we pursued came about through direct recommendations from community board members during our project presentations (described above), akin to snowball sampling. We established formal community-engaged partnerships with three CBOs in the Bronx (BronxWorks), Staten Island (Project Hospitality), and Manhattan (Henry Street Settlement) that expressed both a shared interest in the project objectives and the ability to devote some effort to the collaboration. In explicit recognition of a partnership relationship, memoranda of understanding (MOUs) were collaboratively developed and the CBOs received compensation for their engagement in the project. Specifically, they assisted with recruitment to ensure adequate participation across racial/ethnic and health insurance groups. They also provided feedback on the data collection and recruitment materials, outreach approaches, and settings/arrangements for in-person focus groups. Some examples were providing childcare and adding that information to recruitment materials; identifying locations for in-person neighborhood-based recruitment; and providing facilities in close proximity to other programming activities (for the convenience of community members).
New York Ombuds Programs: New York funds ombuds programs comprising a group of nonprofit advocacy organizations that work independently of the state and health insurance providers (Community Services Society, 2023; Independent Consumer Advocacy Network, 2023; New York State Department of Health Medicaid Redesign Team, 2014). The Independent Consumer Advocacy Network (ICAN) and Community Health Advocates (CHA) ombuds programs provide help accessing and enrolling in insurance; solve problems with healthcare providers, local departments of social services, and insurers; and help file complaints and appeals, including providing representation. Given the alignment of the focus group project on health equity with the goals of these ombuds programs, they shared recruitment materials with their clients.
NYC Democratic Socialists of America (NYC-DSA): The NYC chapter of the Democratic Socialists of America (NYC-DSA) operates a number of branches and working groups organized by ZIP code and topic of interest, including a Healthcare Working Group (HWG) (New York City Democratic Socialists of America, 2022). We made a project presentation to HWG members that resulted in partnering with the working group to disseminate project recruitment materials via email list-servs and at several in-person NYC-DSA events.
Academia/Research Initiatives
CUNY School of Public Health: As an academic research institution, staff at the school of public health (SPH) led this research project, with the valuable and ongoing collaboration of colleagues in the Bureau of Equitable Health Systems at the NYC health department. We employed our expertise in community-engaged research utilizing a mixed-methods study design involving participation from across the five NYC boroughs. In addition to the multidisciplinary community-based recruitment efforts contributed by the various stakeholders (described above), we were able to leverage the favorable status of this large, public institution of higher education to attract study participants from throughout the city (i.e., via institutional communications, networks, and social media). Additionally, we periodically disseminated recruitment materials via the project social media accounts on Facebook, Instagram, and LinkedIn.
Harlem Health Initiative (HHI): The Harlem Health Initiative provides direct support to CBOs that provide services to Harlem residents, in order to foster a strong academic-community relationship though social justice and service-oriented programs (CUNY Graduate School of Public Health & Health Policy, 2024). The HHI hosted the HEAC team to conduct an informational webinar with approximately 40 individual and organizational members of the Harlem community. This event focused on eliciting community input and recommendations for all aspects of the proposed project, from communities to include in recruitment efforts, to health equity issues to be discussed in the focus groups (such as being treated differently from other patients or having “inferior” health insurance), to connections with Harlem and Bronx community boards. Participants distributed recruitment materials via their partner CBOs, and project staff were provided with opportunities for event-based recruitment (see below). Additionally, recruitment documents and materials were disseminated via the HHI community list-servs.
Pandemic Response Institute (PRI): In response to the COVID-19 pandemic’s impact on NYC, the Pandemic Response Institute was created as a partnership between CUNY SPH and Columbia University to support New Yorkers, city agencies, and CBOs in preparing and responding to current and future public health crises (NYC Pandemic Response Institute, 2023). The PRI disseminated recruitment documents and materials through their various CBO partnerships and other NYC community-facing activities.
Business Sector
Despite our extensive, collaborative outreach efforts to include a diverse group of New Yorkers in the HEAC project, there were some racial/ethnic and insurance groups with relatively lower levels of participation earlier in the recruitment phase. In addition to targeted outreach with our CBO partners (described above), we collaborated with Qualtrics, an American-based data management company that provides a variety of services including survey administration and research participant panels. We partnered specifically for assistance recruiting participants from their NYC panels who identified as white and who had either private insurance or Medicaid (Qualtrics, 2023). This was a successful collaboration resulting in 10 focus groups evenly split between participants with private insurance and Medicaid.
On-the-Ground Recruitment in NYC Communities
We employed field-based recruitment efforts, concurrent with the myriad collaborative activities we engaged in with different stakeholders (across the four key sectors), to include New Yorkers from across the city in focus groups on health equity. One category of our on-the-ground activities involved participating in local public events (e.g., tabling) that focused on health and/or social issues. Examples of these events included “Public Health Corps in Your Borough — Fall Festival” (Staten Island and Manhattan), “Lower East Side Community Roundtable,” “Back-to-School Youth Resource Event” (Harlem), “Scan Van for Free Mammograms” (Community Health Action of Staten Island), and “Art in the Parks” (various sites).
We also conducted intensive, targeted direct-to-participant, neighborhood-based outreach to disseminate project recruitment materials in person throughout the five boroughs, specifically focusing on neighborhoods with relatively higher proportions of the demographic characteristics that were under-represented in focus groups conducted to date. This involved accessing the most recent publicly available NYC demographic data from the US Census Bureau and analyzing it by ZIP code to focus street-based recruitment efforts. We then used geographic search tools available through Google maps to identify specific areas/venues within these neighborhoods that might be particularly suitable for outreach. Such sites included commercial shops and restaurants, library branches, community and cultural centers, parks, and other locations frequented by residents.
Participatory Method Generated a Diverse Sample
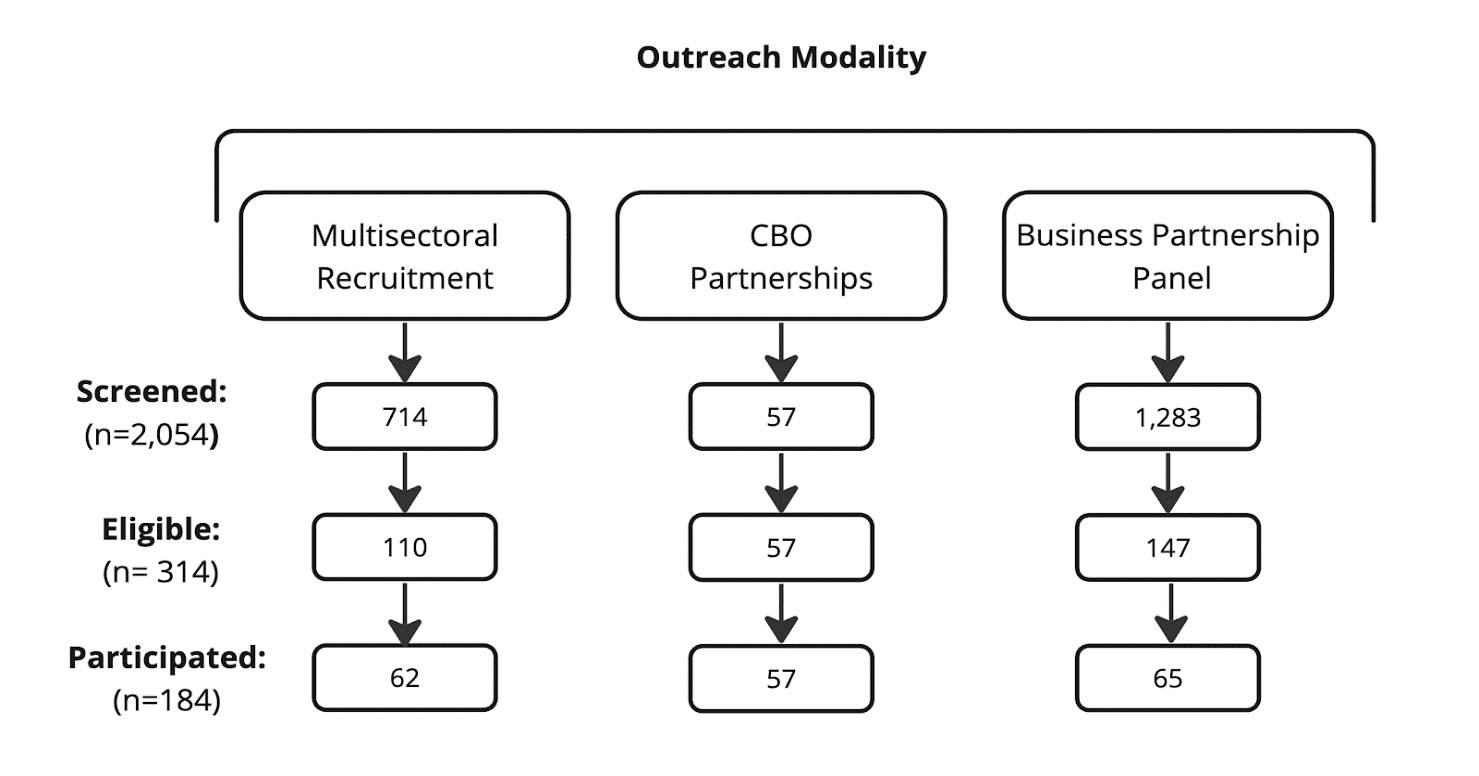
As the focus groups progressed, we analyzed participant characteristics data to identify if there was relatively more or less participation by certain groups as well as by geographic area (borough) of the city. This ongoing monitoring informed our outreach efforts which led to subsequent phases of recruitment (i.e., field-based recruitment, CBO partner and business sector coordination). Ultimately, a combination of strategies was necessary to achieve the diversity of participation essential to understand mechanisms that drive inequitable healthcare experiences and care segregation. The phased recruitment approach allowed us to successfully implement an inherently dynamic project and recruit participants through various outreach modalities. Figure 2 depicts the response to the various outreach modalities employed and Table 1 summarizes the recruitment modality reported by focus group participants. Ultimately, an important measure of our success in recruiting a diverse group of New Yorkers to share their experiences accessing healthcare is the make-up of the sample. As presented in Tables 2 and 3, respectively, there was variation in focus group participants across several key characteristics (sex, age, race/ethnicity, health insurance, and NYC borough of residence) and key informants across various sectors.
__to_eligible_candidates__and.png)
Capturing Diverse Experiences with Inequitable Healthcare
A major strength of qualitative data is how stories of personal experiences help explain and extend our understanding of statistical trends, in people’s own words (“in vivo”). The focus group and key informant findings revealed factors associated with decision-making and experiences accessing healthcare in NYC hospitals. While the complete study results are reported separately, the stratified focus group study design we employed allowed for identifying factors that differed by individuals’ race/ethnicity and type of insurance.
The key focus group themes that related to determining if and where to seek healthcare, and influences on the nature of the care experience (i.e., logistical/structural, interpersonal, provider/facility characteristics, and cost/insurance) exhibited differences by race/ethnicity and insurance. As a result of the multi-sectoral sample recruitment approach employed, we identified important themes related to racist healthcare experiences, as illustrated by the selected sentiments below:
“Sometimes as being a black woman, when you go into these offices, you know, they immediately think you have Medicaid. They immediately have the assumption that you might be less educated. These things all play a role in your health care, you know, it’s part of the social determinants of health.” [AA/B, Private insurance]
“…the first two times that I went that [wasn’t a] provider of color, they rushed through. It was very painful, I was crying, he still didn’t stop.” [AA/B, Private insurance]
“It never even occurred to me that doctors would be racist. I’m just such an idiot about this… But [now] I make it a point to always dress very business casual when I go to the doctor.” [AA/B, Medicaid]
“…then the dynamic is, well, is this [having to wait] happening for everyone who was in the lobby or just people of color, like, you know, you don’t really know how we’re being assigned.” [AA/B, Medicaid]
“People deal with like racist assumptions or some doctors don’t even want to deal with you, they’ll say like, oh this guy’s disgusting, I don’t even want to look at you. But they don’t say that. You feel it. Yeah. Like when you get one of those doctors, I get off the bed. I go somewhere else.” [H/L, Medicaid]
“Yes, skin, like that. He give you the service on how you look. He see you Spanish, Black, a lot of people are white in the hospital. They don’t give the same service to everybody. Everybody go for the same [thing] but he don’t give you the same service.” [H/L, Medicaid]
The relatively few accounts from white and Asian/Pacific Islander (A/PI) participants of being treated differently pertained to having an invisible disability and poor provider communication for non-native speakers, respectively.
With regard to the key informant (KI) interviews, they included representatives from NYC private hospitals, public hospitals, healthcare advocates, and other healthcare-related roles (Table 3). We analyzed specific topics within the themes identified, by KI category, and found that all (or almost all) KIs highlighted the importance of culturally competent/respectful care; Medicaid reimbursement rates; structural barriers to care; and difficulty finding specialist care.
Benefits of and Lessons Learned from a Participatory Study Design
That the HEAC project was supported by the NYC health department is indicative of the agency’s concern with and commitment to addressing inequitable and segregated healthcare in NYC. However, the bureaucratic structure and processes of such a large municipal entity might be expected to inadvertently present challenges to implementing a project involving different community sectors and stakeholders. Thus, partnering with an academic research center leveraged the ability to quickly respond to changes on the ground (e.g., ebb and flow of recruitment, collaborator limitations/needs), which was facilitated by both human- and systems-related factors. First, the collaboration between the health department and an academic partner (department of community health) brought together two public health, mission-driven entities with staff committed to collaboration and community engagement in order to improve public health. While each had its specific skillset, the two key partners were essentially “on the same page” from the outset. The health department conducted data analyses documenting the nature of segregated hospital care in NYC which informed the study design, while the academic partner had a range of pre-existing community-based relationships and expertise with nimble project implementation to respond to the dynamic nature of communities (e.g., field-based outreach, logistics associated with participant incentives, establishing MOUs with CBO partners). Together, we developed the draft data collection instruments, which were then shared with community-based stakeholders and revised to incorporate their feedback.
Forming a multi-year MOU between the academic partner and the health department was a benefit and crucial part of securing the relationship between the two key partners. Fiscal and administrative barriers are often seen as challenges to community engagement and community engaged research (Carter-Edwards et al., 2021). Burdensome paperwork, contract negotiations, and the pace at which the back-and-forth communications happen can have an impact on the relationship itself, the timing for when the work begins, and payments for the work (Wilkins et al., 2023). While there are some administrative hurdles that could not be avoided, we sought to create a more sustainable partnership by establishing an MOU spanning three fiscal years with a maximum budget assigned to each year. The expectations of each party were outlined along with the proposed deliverables for each fiscal year. Creating a multi-year MOU allowed us to avoid annual negotiations and paperwork, and associated work delays or disruptions due to administrative requirements. The partnership allowed for several aspects of the study to work as it did, especially regarding timely engagement with other community stakeholders. The shared leadership led to the achievement of our specific research goals.
The multi-year MOU was also structured so that other projects could be supported by the same MOU with few additions. While the multi-year MOU allowed for continuity within the work, it also met the goal of installing a long-term partnership between two teams at the academic and health department institutions. There are plans to renew the multi-year MOU and expand upon the current work being done. Additionally, work is underway within the health department to educate other teams in creating multi-year MOUs with their community partners in hopes of creating long-lasting and more supported relationships that prioritize community engagement and community-engaged research across the agency.
Although the study’s phased recruitment approach created opportunities for outreach across many partners in the city, we still faced traditional barriers and limitations with this project. We conducted outreach and engaged with a wide variety of participants across our diverse community entities, yet many of these organizations did not reciprocate. Despite numerous attempts, phone calls and emails went unanswered. For some outreach efforts, like with the borough president offices and community boards, it is difficult to measure the impact of their outreach efforts, or the extent to which the outreach they promised occurred. Additionally, the public library systems represent a huge municipal institution across the city. Library resources include language classes, internet access, and educational workshops, and the institutions serve as a place of refuge for many across the city. Not being able to partner with the library systems was a missed opportunity for engagement; however, their policies regarding payment of incentives provided a learning opportunity for future engagement with such entities that have finance-related policies, especially those that serve a vital role in NYC.
Engaging with and recruiting participants with certain racial/ethnic identities and/or insurance statuses required extra efforts. As such, we established formal partnerships with CBOs that served certain communities such as Hispanic/Latinx (BronxWorks) and Asian/Pacific Islander (Project Hospitality, Henry Street Settlement). Likewise, by tapping into the resources available through a business partner, such as Qualtrics, we were able to fill a serious gap in the recruitment of white participants with different insurance statuses.
The next steps of this project include returning to the community to request feedback on the findings of this work. Keeping desegregating health care at the forefront of our dissemination plan and asking what participants see as possible uses for the study findings can broaden our dissemination and strengthen our programmatic and policy initiatives. The work does not end here but will lead to ongoing conversations as we seek to co-create sustainable programs and policies that challenge healthcare segregation and inequities in care (Walker et al., 2022). Data sharing with the community is an important part of supporting this campaign and continued engagement with communities around this work is a key aspect of the dissemination plan. Specifically, our municipal, civil society, and academic research partners have all expressed interest in our presenting the project findings to them to enable their feedback on relevant policy and programmatic recommendations.
Conclusions
This large, qualitative research project both reached out directly to New Yorkers as well as in partnership with various sectors and stakeholders to engage individuals in conversation about their experiences accessing segregated care at public and private hospitals in NYC. Multiple stakeholders engaged in different phases of the project and in different capacities to reach out to and invite participation of New Yorkers from diverse communities throughout the five boroughs. A varied combination of partnerships with different sectors and organizations was employed to achieve the goal of the broadest participation possible to best inform policies and programs focused on eliminating segregated healthcare in NYC.
Acknowledgements
We are grateful to the many individuals and organizations who made valuable contributions to this project. We greatly appreciate our partners, including BronxWorks, Henry Street Settlement, and Project Hospitality, NYC community board members and borough presidents’ staff, and countless other entities that assisted with recruiting a diverse group of participants. We very much appreciate the dedicated HEAC team of outreach workers, focus group moderators, and data analysts. Finally, we are most indebted to the almost 200 New Yorkers who genuinely participated in the focus groups and key informant interviews and shared their healthcare experiences and knowledge with us.
Funding
This work was supported funding from the New York City Department of Health and Mental Hygiene [RF Grant #58814].
Community Boards are comprised of members through a combination of NYC Council nominations and borough president appointees. The City Charter mandates that each Community Board consider the needs of the Community District that it serves and cooperate with, consult, assist and advise elected governmental officials about any matter that “relates to the welfare of the Community District and its residents.” (https://www.nyc.gov/site/brooklyncb1/about/community-boards-explained.page)