Background and Significance
Community resilience, traditionally associated with natural disaster response, has been more recently extended to encompass chronic challenges, community stress, and acute traumas experienced by communities (Bozorgmehr et al., 2023; Ellis et al., 2022; Norris et al., 2008). According to the community coalition action theory (CCAT), coalitions can form in response to threats, as well as by opportunity or mandate (Butterfoss & Kegler, 2012). Thus, community coalitions create a resourced network to foster community resilience in response to chronic threats like structural inequities or acute challenges. A recent and well-documented example is the COVID-19 pandemic, an acute trauma that resulted in disproportionate economic, social, and health burdens in communities of color compared to white communities (Ellis et al., 2022; Marquez et al., 2021).
The CCAT suggests that coalitions develop through stages, from formation to maintenance to institutionalization, and consist of fourteen constructs and twenty propositions (Butterfoss & Kegler, 2012). One theoretic proposition explains that synergistic sharing of resources brings about strategies for comprehensive assessment, planning, and implementation. Community resilience also relies on community resources, such as social capital, communication, community competence, and economic development to adequately respond to challenges (Norris et al., 2008). Norris (2008) also suggests that community adaptive capacities are supported through connectedness and strong relationships between different sectors and organizations in a community. Taken together, resources and partnerships are central to both coalition success and community resilience.
In 2005, the Nevada State Legislature authorized the creation of the Nevada Office of Minority Health and Equity (NOMHE) through Assembly Bill 580 and tied it to an advisory council that reflected the racial-ethnic and geographic diversity of the state. In 2017, NOMHE leadership publicly recognized that the lack of funding and staff support made operating at a basic level difficult (Nevada State Legislature, 2017). The lack of support for NOMHE posed a threat to Nevada’s underserved communities and minority health issues. Minority populations already experienced lower household income, education achievement, and worse health outcomes, such as diabetes and heart disease, compared to white populations (Nevada State Legislature, 2017). Parallel to the efforts to revitalize NOMHE, the Nevada Minority Health and Equity Coalition (NMHEC) was formed to garner community and academic support for NOMHE and to address health disparities in the state. Using the example of the NMHEC, the aims of this article are two-fold. First, we aim to identify networked resources and integrate them into the CCAT to advance an understanding of community resilience. The second aim is to share NMHEC strategies that embed community participation into each CCAT construct.
Methods
Through an analysis of archival documents such as legislative assembly bills, coalition recruitment materials, meeting minutes, and partnership and event evaluation, we describe strategies and resources that fall within the 14 CCAT constructs. Constructs 1–7 describe coalition formation, structure, and processes while the remaining constructs 8–14 relate to the coalition interventions and outcomes. In addition to Table 1, which summarizes CCAT constructs, strategies, and resources needed by the NMHEC, the narrative in the next section describes strategies and resources required.
Construct 1: Stages of Development
The first construct of the CCAT is the stages of development; coalition formation, maintenance, and institutionalization. The impetus for coalition formation was the need for minority health and equity resources. In this construct, resources are political partnerships, civic participation, community action, community engagement, community time, and ideas.
Coalition Formation
Between 2013–15, the Nevada Legislative Assembly gained diverse membership, including African American and Latino elected officials who elevated minority health issues and concerns and questioned why the Nevada Office of Minority Health and Equity (NOMHE) did not have stable funding. In addition to the change in the political landscape, Nevada’s public health community faced challenges presented by health statistics of Nevada’s minority community. Overall, healthcare in Nevada had — and has — numerous issues, but minority communities were left to handle healthcare needs with limited state resources. As a result, community organization representatives began to share common interests and barriers. These events created momentum supporting Assembly Bill (AB) 141 (Assembly Bill (AB) 141, Nevada 79th Session, 2017), written by the late Nevada Assemblyman Odis Tyrone Thompson.
Before the introduction of AB141, the Nevada Department of Health and Human Services commissioned a study to learn what the community needed and wanted from NOMHE and a coalition (Strategic Progress, LLC, 2016). This formative work included five community convenings, a survey, and individual interviews with public health agencies, community-based organizations, nonprofit organizations, business entities, advocacy groups, and academic and community leaders to learn what the community envisioned for NOMHE and a community coalition.
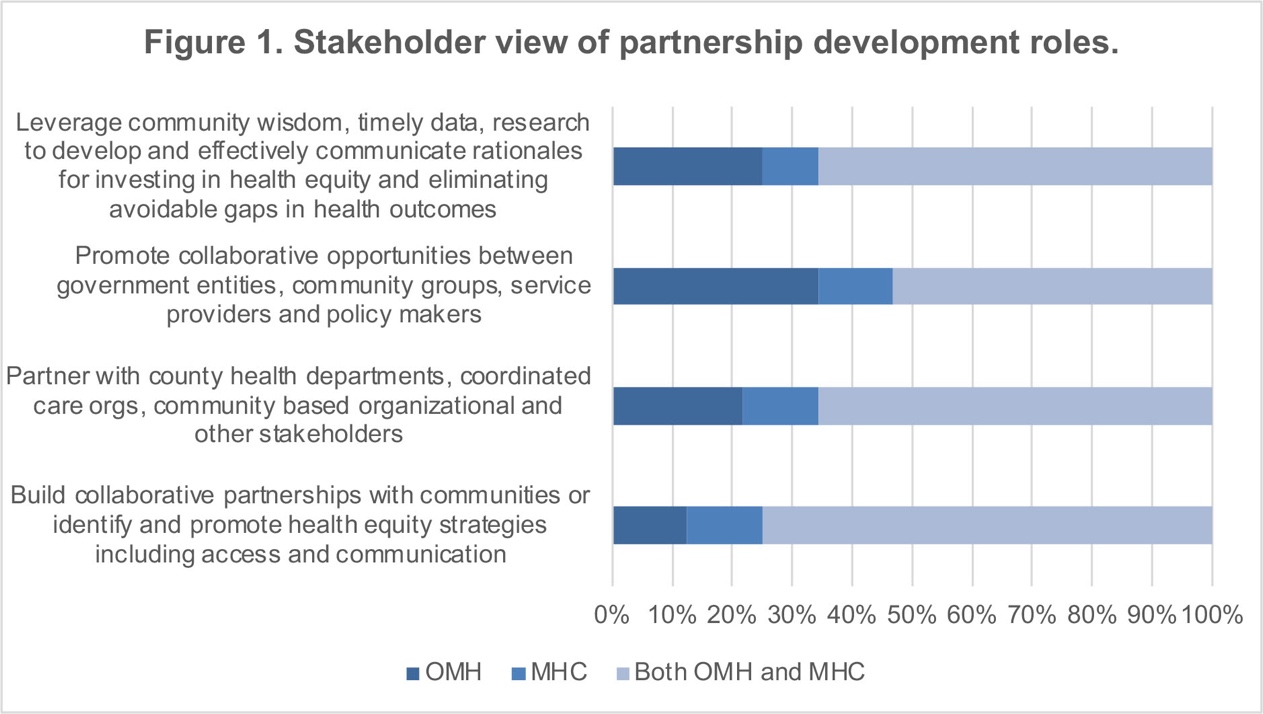
Community engagement was critical to community mobilization in support of AB141, but it also generated ideas and strategies that would inform NMHEC development. Based on survey data from the commissioned report, NMHEC’s initial role was to function as a convener and bring organizations and individuals together around minority health and equity. Survey participants (n=32 organizations, 61.5% response rate), indicated that the Office of Minority Health (OMH) and the Minority Health Coalition (MHC) should work together to leverage resources, promote collaborative opportunities, partner with stakeholders, and collaborate to identify strategies to promote health equity (see Figure 1).

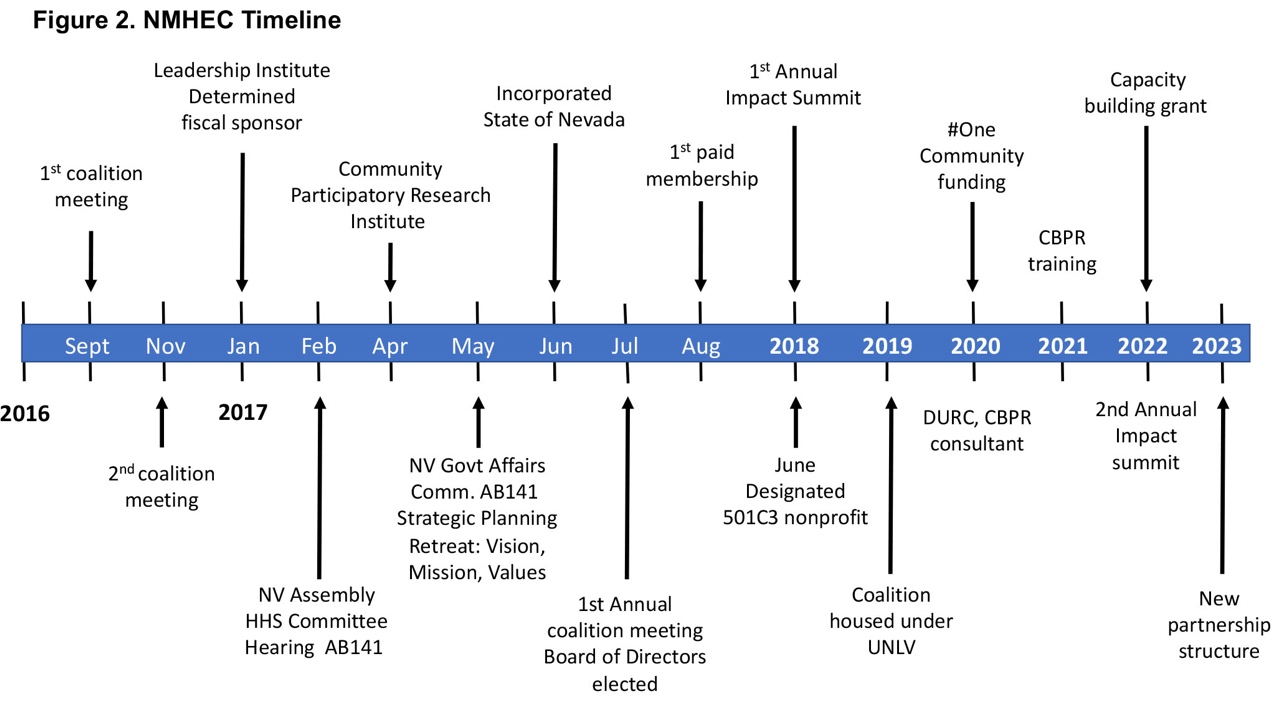
During formation, the coalition gathered concerned stakeholders who experienced equity gaps in programs, practices, and policies across the state. The first year of meetings (2016–17) focused on identifying and developing the NMHEC structure. In 2017, the coalition determined a fiscal agent and submitted its articles of incorporation to the state (see Figure 2).

Coalition Maintenance
Regular meetings were set, and volunteers were identified to serve in leadership capacities. The NMHEC Board of Directors (BOD) volunteers dedicated their time and talents to help build the foundational structure of the coalition. To formalize the coalition’s identity, a series of strategic planning sessions were held where a clear directive emerged: all work and support of the coalition needed to have community voice and input.
This directive led the coalition to adopt a community-based participatory research (CBPR) approach as the coalition framework. This approach, guided by nine principles, centers community experience and knowledge, democratizes the research process, develops a shared leadership structure, and prioritizes issues identified by the community (Israel et al., 2018; Lucero et al., 2024). The BOD secured a series of CBPR trainings for coalition members to lay the framework foundation. The first training occurred in April 2017 (see Figure 2) and continues to be regularly reinforced for NMHEC through training and practices. The most recent CBPR training took place in 2023.
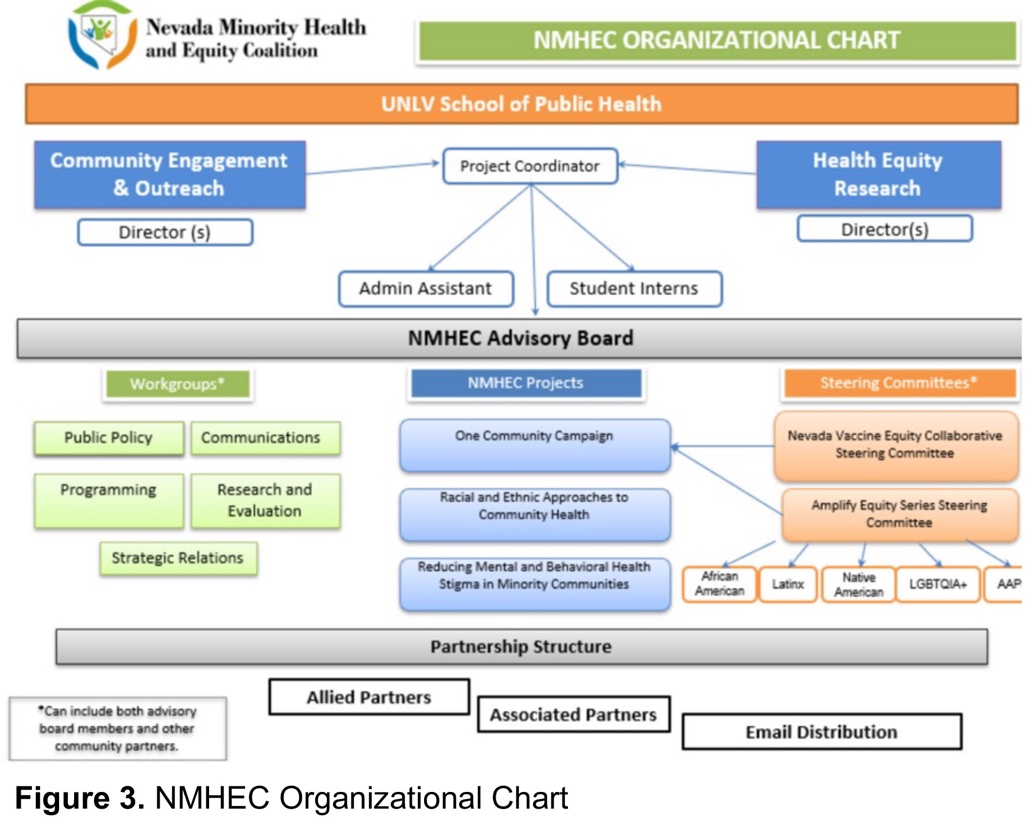
In line with shared leadership, coalition partners and the BOD established the mission and vision. NMHEC’s mission is to “promote the health and well-being of diverse communities by pursuing research, capacity building, and advocacy that recognizes the unique cultural and linguistic differences of Nevadans” (Nevada Minority Health & Equity Coalition, n.d.). The formation stage laid the groundwork for setting coalition priorities: 1) Building capacity; 2) Informing policy; and 3) Advancing health disparities research. Workgroups were developed to facilitate programming in these priority areas, specifically public policy, strategic relations, programming, communication, and research and evaluation (see Figure 3). Each workgroup supports critical programming of the coalition, including member engagement, branding, coalition evaluation, informing policy, and grant writing. In addition to workgroup meetings, quarterly partner meetings are held to provide opportunities for engagement and networking among members.

Coalition Institutionalization
The institutionalization of coalition work resulted in long-term sustainability. The lead agents (see Construct 3) saw the fragility of an organizational entity that did not have full support and institutionalization. Thus, finding a supportive and resourceful environment for the coalition was imperative.
While the University of Nevada Las Vegas (UNLV) School of Public Health supported coalition development by helping with formative work and providing coalition administration, the push for community oversight led the coalition to find a fiscal home. Between 2017–18, the NMHEC submitted its articles of incorporation and became a non-profit 501c3 (see Figure 2). At this time, a community organization stepped up to fulfill the role of fiscal agent to the maturing NMHEC. This arrangement allowed the coalition to use the fiscal agent’s administrative structure to do contract work, receive donations, and apply to funding opportunities. The institutional support was critical in the early stages of development but quickly found the coalition outgrowing the mission of the fiscal agent.
In 2019, the coalition shifted from being a standalone 501c3 to an office within the UNLV School of Public Health. The decision was not easy. Coalition members expressed fears that UNLV would end up taking over, but the coalition has remained community focused and the move has been beneficial in many ways. In the four years at UNLV, the coalition has received institutional commitments such as a dedicated administrative staff, research assistants, robust human resources, access to the institutional review board, and financial and grant services such as grant submission assistance and contracting. Some challenging areas are hiring requirements and navigating university policy changes and procedures like using gift cards as participant incentives and payment to contractors. Being committed to the CBPR framework, NMHEC bridges academic research with community needs and builds capacity among diverse members to address ongoing and emergent issues.
Construct 2: Community Context
Coalitions are heavily influenced by contextual factors throughout all stages of development, according to CCAT proposition 3 (Butterfoss & Kegler, 2012). Community context can include a variety of factors such as a history of collaboration, political landscape, community representation, structural inequities, and available resources. Resources used by NMHEC in this construct are civic participation, research skills, data, institutional collaborations, and community knowledge.
An element of community context is understanding the political climate. In 2019, Nevada became the first state in the U.S. to seat a majority-female legislature and in 2021 had the highest percentage (60%) of female legislators (Research Division Legislative Counsel Bureau, 2023). According to the National Congress of State Legislatures (NCSL), in 2020, about 30% of NV Legislatures identified as Black, Hispanic, Asian/Pacific Islander, and multiracial (NCSL, 2020). Most female and non-white legislative members are affiliated with the Democratic party, even though the state leans Republican. The political leaning is important as Democrats tend to give more attention to underrepresented populations. That said, NMHEC has worked to include elected officials from both sides of the aisle because “sustainability of a new OMH and MHC must be a legislative priority and championed not only by the Black and Latino caucus but also by all legislators” (Strategic Progress, LLC, 2016, p. 6). Understanding the legislative political makeup and constituent priorities helps identify common ground and political allies.
Nevada communities vary in demographics, geography, and political orientation. Between 2010 and 2020, Nevada’s population increased by 15%, making it the fifth fastest-growing state in the U.S. (Girnus, 2021), with a 69% diversity index in 2020, up from 62.5% in 2010 (U.S. Census, 2023). By comparison, in 2020 the U.S. had a 61.1% diversity index score. The diversity index asserts that if two people were randomly chosen, there would be a 61% chance of each being from a different racial/ethnic background (U.S. Census, 2023).
The diversity index increase is because much of the population growth has been among people of color. Based on the latest census, Nevada’s population is comprised of 30% Latino/Hispanic; 11% Black/African American; 9% Asian; 2% Native American; and 5% of two or more races (U. S. Census, 2020). While the state’s racial and ethnic diversity is increasing overall, most of the growth remains in Clark County (Las Vegas) and Washoe County (Reno). Other Nevada counties have seen modest increases, including the rural areas (America Counts Staff, 2021).
With varying demographics, upstream barriers to health and social equity become more visible. For example, about 14% of the state’s population lives in poverty, 30% speak a language other than English at home, and 14% of the population does not have home internet access (U. S. Census, 2020). During the COVID-19 pandemic, language resources were sparse and most services shifted to remote environments, leaving those without internet or proficient English behind. Among the population under 65 years old, 9% live with a disability, and 14% do not have health insurance (U. S. Census, 2020). In Northern Nevada, 50.6% of patients diagnosed with COVID-19 identified as Hispanic and were significantly more likely to be uninsured and to live in low-income communities as compared to their non-Hispanic counterparts (Antwi-Amoabeng et al., 2021). These public statewide data provide a snapshot of the community context. Each Nevada community has a different demographic, socioeconomic, and local politics that dictate public funding, priorities, attitudes, and support (Bozorgmehr et al., 2023).
Construct 3: Lead Agency/Convener Group
The CCAT asserts that coalitions form when a lead agency or convener group supports the formation stage. The coalition needed resources such as organizational links and cooperation, trusted sources of information, social support, relationship-building skills, and communication (Table 1) to cement itself as a health equity convener and leader. NMHEC informs, develops, and implements culturally informed approaches. As problems or issues are identified, NMHEC engages key community stakeholders to inform strategies, which aligns with 77% of stakeholder expectations that the NMHEC increases awareness, education, and outreach to address racial/ethnic minority health and health disparity problems throughout the state (Strategic Progress, LLC, 2016). This requires a vast community network from which to pull expertise and reach to disseminate information.
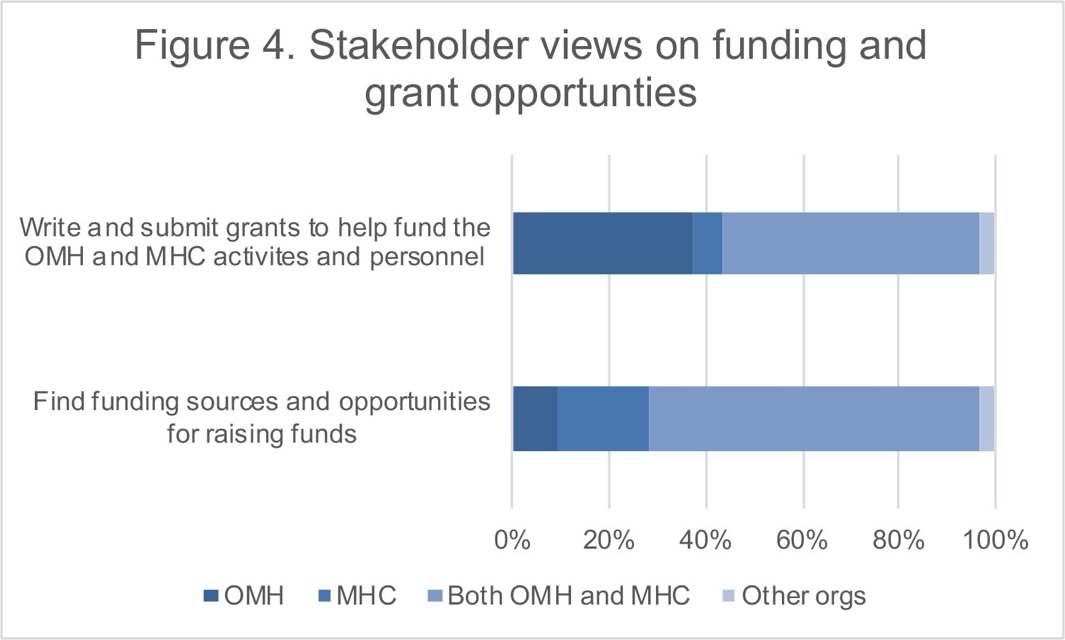
Another directive of the coalition is to find funding sources and opportunities, and write and submit grants for health equity research and sustainability (see Figure 4, Strategic Progress, 2016). Grant collaboration requires relationship building and trusted, transparent communication streams.

When grants are written, communities are included in the process and any subsequent funding to do the work. Collectively, the coalition believes that community voices are needed in the decision-making process and day-to-day activities.
Construct 4: Coalition Membership
Aligning outcomes among diverse community partners is necessary for active engagement in coalition work. Community gatekeepers, community members committed to the issue, and a broad constituency of diverse groups and organizations must be recruited (CCAT propositions 6, 7, and 8). Building coalition membership requires community knowledge, relationship-building skills, professional networks, social support, collective efficacy, trusted sources of information, and organizational links and cooperation (Table 1).
NMHEC grew from a committed few with an informal membership structure, to many with a formal partnership structure with different levels of engagement. To date, NMHEC membership consists of 33 individual and organization partners. NMHEC leaned on coalition members with process expertise (authors 2-8) to develop a successful membership structure. The NMHEC sought counsel from the Detroit Urban Research Center (DURC), part of NMHEC’s professional network. Dr. Barbara Israel, DURC’s director and community-based research expert, helped NMHEC understand DURC’s function, membership structure, and the specific successes and barriers to process implementation. Considerations included individual or organizational membership, membership levels and benefits, commitments, expectations, and tracking and evaluating processes. After much consideration, the following describes the final membership structure.
First, the advisory board decided to call members partners. This term provided a more inclusive feel and encouraged engagement. Second, it was decided that coalition members should include individual members and organizations. Thus, memberships represent academic, civic, private, and community organizations serving Nevada’s diverse populations. Next, the NMHEC settled on creating a tiered membership — Allied and Associated partners, which allowed for variations in levels of engagement to accommodate the diverse groups. In addition to the two partnership levels, there is an option for email notification only which provides a way for individuals or organizations to stay informed even if they are not ready for a larger commitment. Allied partners are organizations or individuals who commit more time to the coalition through participation in workgroups or steering committees and, in return, also receive additional benefits such as being prioritized for interns and funding opportunities. Associated partners are those who have less time but still want to be involved with NMHEC. While membership is free, agencies do have to apply through an online application process.
Construct 5: Operations and Processes
Internal and formal processes are needed to determine and deploy resources equitably. Resources used to develop operations and processes for NMHEC functioning and community resilience are communication and information sharing, leadership skills, shared and formalized decision-making, conflict management skills, interpersonal relationships, infrastructure development, equity of resource distribution, and collective efficacy.
The NMHEC has quickly grown, necessitating the development of the coalition’s structure and everyday operational procedures while ensuring transparency. Due to the focus on minority health and equity, there was an intentional dialogue about procedural and recognitional justice. More specifically, decisions were made to be inclusive in the decision-making process and to respect diverse stakeholders and knowledge systems (York & Yazar, 2022). An operation manual that details day-to-day operations of the coalition, and operations of the advisory board, working groups, and steering committees, is being developed,
Under the guidance of the DURC, NMHEC developed a set of operational norms. To develop these norms, DURC facilitated a series of breakout sessions with NMHEC members based on the prompt, “What are the characteristics of successful coalition groups?” The resulting norms are presented in Table 2. These norms are reviewed during the new member and new board member orientation and can be found in the strategic plan and orientation manual.
A set of procedures for day-to-day functions was developed to support transparency, accountability, and continuity in the event of staffing changes. Every two years, the NMHEC updates its strategic plan which requires a review of the priority pillars of the coalition, goals, objectives, mission, and vision of the coalition. Any changes will subsequently require updates to the evaluation and monitoring of workgroup and steering committee metrics, activities, and timelines. Some additional examples of processes that have been set up are procedures about how meetings should be held (e.g., agenda setting, setting up a consistent schedule), communication efforts, evaluation and monitoring, publication guidelines, funding requests, grievance procedures, and conference/event planning.
Since the coalition values shared decision-making, it is important to the NMHEC that coalition members have consistent pathways for bi-directional communication. There are several methods to ensure that members are included in the process. First, the NMHEC has established workgroups and steering committees that are not exclusive to the advisory board, and depending on the membership level, participation is expected. There are five workgroups that each have a specific focus (see Figure 3). The workgroups decide on their specific activities and NMHEC staff work with the groups to create annual plans and track their progress and outcomes. This information is then shared with the advisory board and coalition membership at large. The success of these workgroups depends on providing staffing support to assist with scheduling, creating the agenda, taking notes, and following up on action items that emerge from the meetings. Each workgroup is chaired by a member of the advisory board and can be co-chaired by a coalition member. These workgroups are also able to submit requests for financial assistance for projects to the advisory board. The advisory board votes on requests as funds are available. The coalition has aimed to set aside a set amount of funds each year to provide some support. The NMHEC feels financial resources are a demonstration of workgroup support.
Steering committees are like workgroups but were created to support specific grant-funded projects. The initial steering committees were developed based on grant aims to increase culturally specific materials regarding COVID-19. Currently, there are five steering committees (African American, Latinx, Asian/Pacific Islander, Native American, LGBTQIA+), which are staffed by NMHEC staff and chaired by a coalition or advisory board member. Each committee also works to develop an annual work plan with specific activities and outcomes. These plans are shared with the advisory board and community at large.
Finally, outside of the advisory board, workgroups, and steering committees, there is a larger communication strategy to keep members of the coalition and the community informed. Regular communication with coalition members occurs primarily through email updates and quarterly meetings. Email updates consist of bi-weekly community announcements, semi-annual newsletters that highlight coalition work, and other timely updates on community occurrences or responses to local or national events. Quarterly meeting agendas have time built in for member check-ins and updates, workgroups and steering committees provide updates, and speakers are invited to share information on specific topics, and/or training. The coalition is also active on social media, regularly posting to Facebook, X, Instagram, and LinkedIn.
Construct 6: Leadership and Staffing
Building on resources from Construct 5, the NMEHC leadership is uniquely made up of faculty and administrative faculty from the School of Public Health and community leaders with experience in CBPR, the development of public health programs, and years of working in the community. Each member of the team contributes their skills and expertise. Resources required for Construct 6 include leadership and roles, enacted social support, collective efficacy, resource management, data, research skills, and partnership-building skills (Table 1).
The organization structure has gone through iterations, with the most recent presented in Figure 3. The NMHEC advisory board is in the leadership position and direct the coalition’s operations and priorities. Staffing is provided by the UNLV School of Public Health. They provide the coalition with administrative staff support and student interns. Two directors, both UNLV faculty, oversee either Health Equity Research or Community Engagement and Outreach under the direction of the advisory board.
Initially, NMHEC was governed by a board of directors, which changed into an advisory board when moving under the UNLV umbrella. This change reduced the burden of the board as they no longer had fiscal responsibility over the coalition. The 13-member advisory board (including authors 2–7) consists of a diverse makeup representing various racial/ethnic groups, organizations, disciplines, and geographic regions of the state. Workgroups and steering committees are supported by UNLV faculty and from other schools across the state and community organizations.
Construct 7: Structure
A delineated organizational chart that includes formalized roles and responsibilities provides a high-level workflow under which activities occur or decisions are made. NMHEC found that this approach helped with decision-making, power-sharing, accountability, and setting clear expectations. Thus, roles and responsibilities were created for key leadership members, staff, advisory board members, chairs, and co-chairs of different committees.
For NMHEC, the staffing team provides oversight of day-to-day coalition activities, develops and submits grant applications, manages the coalition budget, and oversees grant implementation. The project coordinator supports day-to-day coalition activities such as monitoring the coalition email account and social media, coordinating all meetings, and providing support as needed. The advisory board identifies coalition priorities, provides input on the structure and function of the coalition, including strategic planning, and attends meetings and trainings. Chairs and co-chairs lead the efforts of the various committees. Working closely with the project coordinator to set agendas, facilitate the meetings, and support each of the groups in developing committee activities in alignment with the coalition’s mission, vision, and strategic goals. Workgroup members support the implementation of strategic priorities of the coalition and undertake activities to accomplish the goals. Steering committee members serve as advisory committees for funded projects and non-funded initiatives. Workgroups and steering committees are made up of advisory board members, and associated, and allied partners.
Construct 8: Pooled Member and External Resources
Pooling member and external resources is essential to coalition development and the mutual benefit of all partners. NMHEC membership is rich with resources such as social support, community action, grant writing skills, evaluation skills, data interpretation skills, and professional and social networks. The NMHEC application and annual surveys ask about partner expertise and interests.
The UNLV School of Public Health has invested in the NMHEC by providing administrative and human resources support — two essential elements for any large center. This investment, along with the expertise of partners, results in the ability to submit grant applications. NMHEC does not have an independent budget, rather, funds are awarded through UNLV grants and contracts. Each grant or contract has an accompanying scope of work that partners help complete. Partners are funded for their time and effort in the development, implementation, and evaluation of work conducted. For instance, NMHEC received COVID-19 funding to support the grant efforts for risk mitigation and later vaccination efforts in some of the hardest-hit communities. Partners were funded to strategize ways to provide culturally and linguistically appropriate education in their communities and disseminate final information. Partner expertise, time, and commitment, as well as professional and social networks, are cherished resources.
Construct 9: Member Engagement
Grounded in CBPR, NMHEC values are centered around community engagement, relevance of our work, and collaboration. Coalition investment is centered around an engaged membership, and associated resources are social support, a sense of community, equity of resource distribution, and communication. Sustaining membership is an ongoing activity, such as through direct participation in workgroups and steering committees. These meetings create spaces of collaboration both within coalition activities and among members.
Furthermore, more direct opportunities are available for member engagement and participation in the different workgroups and steering committees (see Figure 3). Steering committees that are not based on grant funding are guided and informed by the members themselves. Thus, activities are designed to be member-driven which means each group collectively decides what issues and priorities are important to work on. For instance, the Latinx steering committee has prioritized conducting a needs assessment with the Nevada Hispanic/Latinx community as the most recent was conducted over 13 years ago.
Another approach to sustaining partner engagement is to administer a member survey annually that helps inform priorities based on community concerns. The survey helps identify what is working or what might not be working within the coalition and opportunities to identify capacity-building efforts that should be focused on throughout the year.
Construct 10: Assessment and Planning
Careful assessment and planning can facilitate the successful implementation of activities, projects, and programs. The first significant step was to develop a coalition strategic plan. Several strategic planning sessions were held with coalition members to develop a mission and vision statement. Then, goals were carefully crafted and aligned with strategic objectives and measurable activities. During the strategic planning sessions, particular attention was paid to capacity, available resources, and setting both short and long-term activities for the coalition. Technical assistance was provided to each workgroup and steering committee to develop measurable activities.
With support from the advisory board, the research and evaluation workgroup developed an evaluation plan that considered both formative and summative components. Process activities were carefully connected to short and long-term outcomes. Ongoing monitoring every quarter allows NMHEC to identify challenges, pivot as needed, hold members accountable, and provide ongoing reporting to board and invested stakeholders. Finally, the strategic plan and evaluation framework aids in making critical decisions throughout the year, such as what activities to prioritize. Resources used here are flexibility and creativity, leadership and skill, and grant writing and evaluation skills.
Construct 11: Implementation of Strategies
NMHEC acknowledges that addressing health disparities is a continuous effort and is committed to developing strategies and interventions across systems. This requires the resources of shared decision-making, grant writing skills, and evaluation skills. Strategies and efforts supported by NMHEC revolve around building capacity, advancing health equity research, and informing policy. Focusing on these pillars is the foundation for more long-term structural changes to policies, practices, and programs. A primary strategy is employing the CBPR approach in all NMHEC endeavors. This enables partners to work together to identify research to practice gaps and co-produce knowledge toward system-level change (Israel et al., 2017). Working with partners who are also community members provides a pathway to guide appropriate strategies for that community. As noted, early coalescing around AB141 at the start gave the coalition momentum. Additionally, while building responses to COVID-19 drove countless hours of work, it created an opportunity to work side-by-side with community partners on something that touched everyone so gravely. It allowed partners to build solidarity, community trust, and self-efficacy.
Construct 12: Community Change
Through shared goals and coordinated efforts, coalitions have been successful in identifying and affecting community-level changes on a variety of issues (Bigland et al., 2020). Responsible information sources, critical reflection, and problem-solving were essential for community change. As a reminder, the NMHEC is not focused on health-specific outcomes. Rather, its focus is on health equity and social justice. Therefore, community change has occurred through education and training, community engagement, and increasing knowledge of resources. An example of education and awareness is the misinformation toolkit (Smith et al., 2022). This 16-page toolkit covers the definition of misinformation, how to identify it, how to stop the spread, and tips on how to talk about misinformation. This document was developed using plain language communication to reach the broadest audience possible (Smith et al., 2022). Lastly, a state-wide community resource guide has been curated and is maintained by NMHEC. The guide provides searchable information on health and social resources by population (e.g. children, Asian populations), need (e.g. housing, food, employment), and health concerns (e.g., communicable diseases, respiratory health). Overall, the network of community partners serves as a resource for each other thereby increasing the community’s ability to impact social and health issues across the state.
Construct 13: Health and Social Outcomes
An indicator of coalition effectiveness is the improvement in social and health outcomes. NMHEC focuses on the pillars of building capacity, advancing health equity research, and informing policy that requires the resources of political and industry partnerships and grant development and evaluation skills. Three projects — #Onecommunity, Health Equity and Literacy Initiative, and Vaccine Health Equity Initiative — illustrate how the three pillars are prioritized. Using CBPR, the coalition engaged in a program to slow the spread and reduce health inequities of COVID-19 in Nevada’s most at-risk populations. The #OneCommunity project partnered with 10 communities to gain insight into how COVID-19 fractured the social and economic foundations. Through focus group discussions, appropriate messaging that covered information about the virus, masking, and vaccinations was developed and packaged into toolkits for each priority population. Community members themselves steered the development of linguistically and culturally inclusive messaging that accounts for their realities and lived experiences. This laid the foundation for the Health Equity and Literacy Initiative seeks to increase organizational health literacy, and building capacity, at four federally qualified health centers in Las Vegas, Nevada, to promote the delivery of healthcare that is consistent with National Culturally and Linguistically Appropriate Service standards. As part of NMHEC’s commitment to advancing health equity across the state of Nevada, the Vaccine Health Equity Initiative (VHEI) aims to increase COVID-19 vaccination rates among underserved and underrepresented communities. To address disparities that contribute to vaccine uptake, the work of VHEI is to provide accurate, evidence-based information about COVID-19 vaccines while addressing community concerns and empowering individuals to make informed decisions about their health.
Construct 14: Community Capacity
CBPR and CR is necessary to building community capacity in coalitions, but how to accomplish it is limited in the extant literature (Schweinhart & Raffle, 2021). NMHECs commitment to community capacity is based on the principle that we can do more if we work together. Thus, a primary goal of the coalition is to build the research capacity of partners to respond to community concerns realized by collective efficacy and capacity-building resources. In 2021, funding was secured to develop a “Building Capacity” series to increase community and organizational capacity, build social capital, and prepare members for dealing with other social and health issues in the future. From June 2022 to March 2023, we held a series of live workshops on a variety of topics that aim to build the capacity of community organizations to address health disparities in Nevada. A few topics addressed in the series are building data capacity, community organizing, advocacy, and grant writing among others. Initially, the workshops were conducted synchronously on Zoom and recorded for later access. After the initial session, the live workshops were adapted into on-demand courses so that the content would be available for convenient viewing. Workshops are recommended for anyone engaging in health equity work.
Discussion and Conclusion
Using the CCAT and community resilience theory, we provide strategies and resources regarding the formation and maintenance of the Nevada Minority Health and Equity Coalition. The CCAT and community resilience require partnership. In the case of NMHEC, partnerships were developed using the community-based participatory research (CBPR) approach. Studies have suggested that the integration of a CPBR framework working alongside coalition partners provides a strategy for translational research and community change. Community resilience and adaptive capacity are necessary to redress health inequities, a chronic threat in minority communities. However, there is limited peer and non-peer-reviewed work that explains the intricacies of what forming a coalition and partnerships looks like in practice. Our experience suggests that the confluence of CCAT and community resilience provides an actionable framework to develop and sustain coalitions that can identify and address local concerns. Here are some of our lessons learned.
Coalition development can be messy. No one framework can explain all the intricacies of developing a coalition. Seek expertise and mentorship from those who have done the work to guide you through the process.
Invest in relationship building. Coalition work can’t be done without people. Building trust and relationships requires an investment of time and effort. It requires establishing open communication channels, identifying common interests, remaining open-minded, sharing ownership, and a willingness to self-reflect.
Identify allies early. Learning who your allies are early can help enhance the ability to get the resources needed to conduct coalition work.
Define your purpose and meet with purpose. A clearly defined purpose allows you to focus on identified priorities. Maintaining engagement requires you to meet purposefully and have a clear agenda and action items for each meeting.
Adaptability and flexibility are key. Coalition work requires adaptability and flexibility to pivot activities and resources as needed. We must be cognizant that efforts may change and evolve based on community input.
Be mindful of power dynamics. Develop rules of engagement that help keep power dynamics at bay. Develop a set of operational norms. These guidelines can help establish clear roles, responsibilities, and expectations early on.
Continuously consider capacity. Many ideas can be generated when developing coalition work. Always reflect on your capacity (e.g., time, skills, manpower) to get the job done. You must continuously prioritize and know it’s okay to say no.
Develop an operation manual. Developing a coalition requires much planning, from scheduling meetings and setting agendas to the development of communication plans. Establish a living document to document how decisions are made and how day-to-day processes should be done. Update the manual regularly.
Secure stable funding. Seek stable funding and grant-funded opportunities. Stable funding can support dedicated staff to help run day-to-day activities. Meanwhile, grant-funded opportunities help support the development of interventions that support the communities you work with.
Identify measurable outcomes. Begin with a strategic plan with goals, objectives, and activities that align with the coalition’s mission and vision. All activities should be measurable. Measurable outcomes support informed decision-making, enhance accountability, and demonstrate impact.
Regularly evaluate, monitor, and reflect on progress. Set up an evaluation plan that monitors formative and summative measures. A logic model can facilitate the process of identifying who is responsible, needed activities, quantifiable outputs, and measurable outcomes and impact. Regularly evaluate and monitor progress to identify successes and areas needing improvement that can be adjusted to reach desirable outcomes.
Navigate conflict constructively. Not everyone is always going to get along. That is expected. Consider developing a process to navigate partner conflicts that includes how conflicts can be reported, a review process, and timelines in which reviews and resolutions should occur.
Translate data into action. Take a broad perspective on how data can be translated into action to advance science, change the environment, or inform policies, practices, and systems.
Disseminate what you learned. Dissemination should target diverse stakeholders and be adapted accordingly. Develop a dissemination plan that defines the purpose, determines the target audience, selects the most appropriate format, and tailors the information to the intended audience.